Division of Vascular Surgery and Endovascular Therapy, Michael E. DeBakey Department of Surgery, Baylor College of Medicine, Houston, Texas.
Department of Biostatistics, University of North Carolina at Chapel Hill, Chapel Hill.
JAMA Netw Open. 2022 Mar 1;5(3):e223424. doi: 10.1001/jamanetworkopen.2022.3424.
Valid risk stratification schemes are key to performing comparative effectiveness research; however, for chronic limb-threatening ischemia (CLTI), risk stratification schemes have limited efficacy. Improved, accurate, comprehensive, and reproducible risk stratification models for CLTI are needed.
To evaluate the use of topic model cluster analysis to generate an accurate risk prediction model for CLTI.
DESIGN, SETTING, AND PARTICIPANTS: This multicenter, nested cohort study of existing Project of Ex Vivo Vein Graft Engineering via Transfection (PREVENT) III clinical trial data assessed data from patients undergoing infrainguinal vein bypass for the treatment of ischemic rest pain or ischemic tissue loss. Original data were collected from January 1, 2001, to December 31, 2003, and were analyzed in September 2021. All patients had 1 year of follow-up.
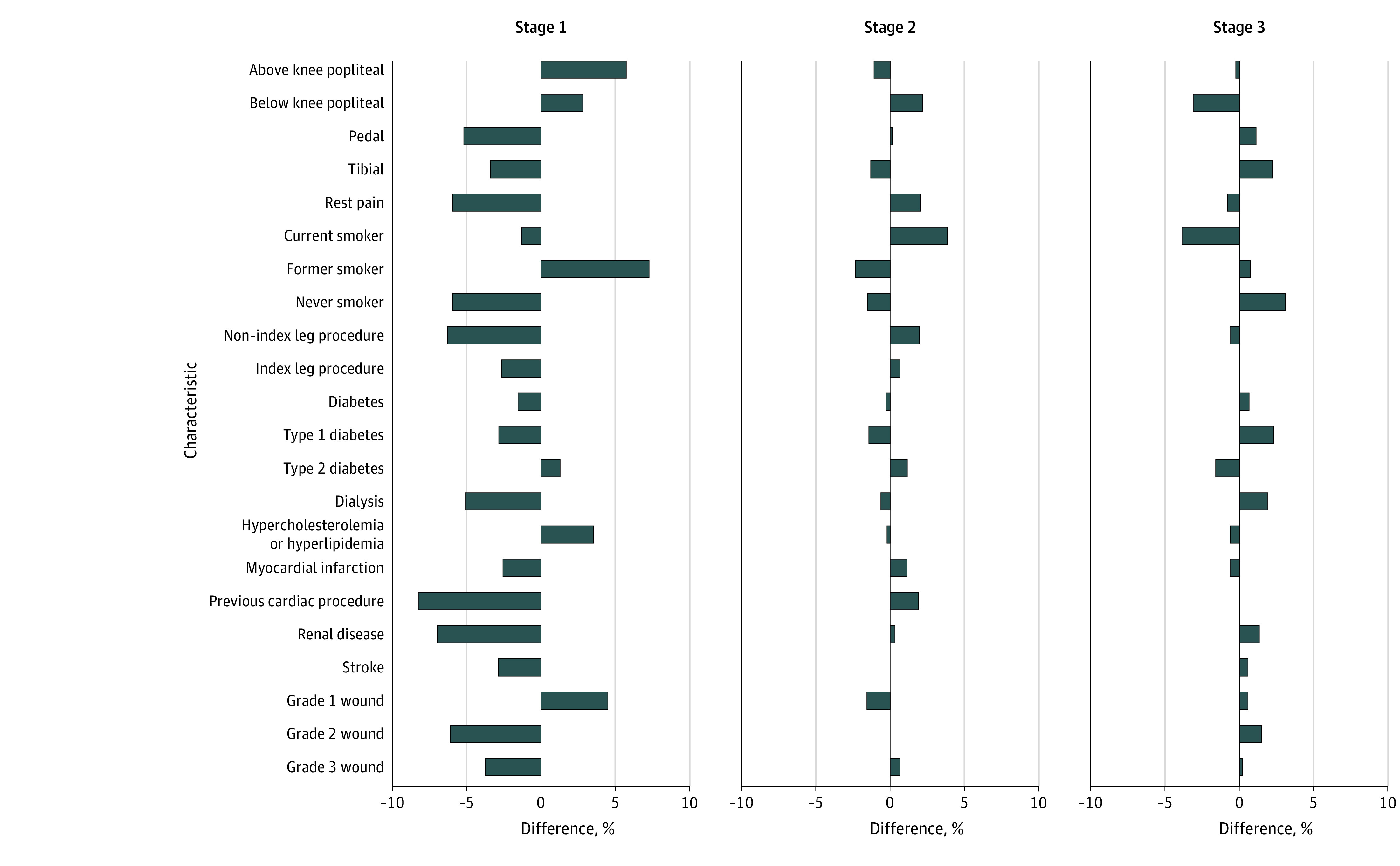
Supervised topic model cluster analysis was applied to nested cohort data from the PREVENT III randomized clinical trial. Given a fixed number of clusters, the data were used to examine the probability that a patient belonged to each of the clusters and the distribution of the features within each cluster.
The primary outcome was 1-year CLTI-free survival, a composite of survival with remission of ischemic rest pain, wound healing, and freedom from major lower-extremity amputation without recurrent CLTI.
Of the original 1404 patients, 166 were excluded because of a lack of sufficient feature and/or outcome data, leaving 1238 patients for analysis (mean [SD] age, 68.4 [11.2] years; 800 [64.6%] male; 894 [72.2%] White). The Society for Vascular Surgery Wound, Ischemia, and Foot Infection grade 2 wounds were present in 543 patients (43.8%), with rest pain present in 645 (52.1%). Three distinct clusters were identified within the cohort (130 patients in stage 1, 578 in stage 2, and 530 in stage 3), with 1-year CLTI-free survival rates of 82.3% (107 of 130 patients) for stage 1, 61.1% (353 of 578 patients) for stage 2, and 53.4% (283 of 530 patients) for stage 3. Stratified by stage, 1-year mortality was 10.0% (13 of 130 observed deaths in stage 1) for stage 1, 13.5% (78 of 578 patients) for stage 2, and 20.2% (105 of 521 patients) for stage 3. Similarly, stratifying by stage revealed major limb amputation rates of 4.2% (5 of 119 observed major limb amputations in stage 1) for stage 1, 10.8% (55 of 509 patients) for stage 2, and 18.4% (81 of 440 patients) for stage 3. Among survivors without a major amputation, the rates of CLTI recurrence were 9.2% (11 of 119 observed recurrences in stage 1) for stage 1, 24.9% (130 of 523 patients) for stage 2, and 29.6% (132 of 446 patients) for stage 3.
The topic model cluster analysis in this cohort study identified 3 distinct stages within CLTI. Findings suggest that CLTI-free survival is an end point that can be accurately and reproducibly quantified and may be used as a patient-centric outcome.
有效的风险分层方案是进行比较效果研究的关键;然而,对于慢性肢体威胁性缺血(CLTI),风险分层方案的效果有限。需要改进、准确、全面和可重复的 CLTI 风险分层模型。
评估主题模型聚类分析在 CLTI 中的应用,以生成准确的风险预测模型。
设计、设置和参与者:这项多中心、嵌套队列研究使用了现有的 Project of Ex Vivo Vein Graft Engineering via Transfection (PREVENT) III 临床试验数据,评估了接受下肢静脉旁路手术治疗缺血性静息痛或缺血性组织丧失的患者的数据。原始数据收集于 2001 年 1 月 1 日至 2003 年 12 月 31 日,于 2021 年 9 月进行分析。所有患者均有 1 年的随访。
对 PREVENT III 随机临床试验的嵌套队列数据进行了有监督的主题模型聚类分析。给定固定数量的簇,使用数据来检查患者属于每个簇的概率以及每个簇内特征的分布。
主要结果是 1 年的 CLTI 无复发生存率,是缓解缺血性静息痛、伤口愈合和免于主要下肢截肢且无 CLTI 复发的复合结果。
在最初的 1404 名患者中,有 166 名因缺乏足够的特征和/或结局数据而被排除,1238 名患者被纳入分析(平均[标准差]年龄为 68.4[11.2]岁;800[64.6%]名男性;894[72.2%]名白人)。543 名患者(43.8%)存在外科血管学会伤口、缺血和足部感染 2 级伤口,645 名患者(52.1%)存在静息痛。在队列中确定了 3 个不同的阶段(1 期 130 名患者,2 期 578 名患者,3 期 530 名患者),1 年的 CLTI 无复发生存率分别为 1 期 82.3%(130 名患者中的 107 名)、2 期 61.1%(578 名患者中的 353 名)和 3 期 53.4%(530 名患者中的 283 名)。分层后,1 年死亡率为 1 期 10.0%(130 名观察死亡患者中的 13 名),2 期 13.5%(578 名患者中的 78 名),3 期 20.2%(521 名患者中的 105 名)。同样,分层后显示 1 期主要肢体截肢率为 4.2%(119 名观察到的主要肢体截肢患者中的 5 名),2 期为 10.8%(509 名患者中的 55 名),3 期为 18.4%(440 名患者中的 81 名)。在没有主要截肢的幸存者中,CLTI 复发率为 1 期 9.2%(119 名观察到的复发患者中的 11 名),2 期 24.9%(523 名患者中的 130 名),3 期 29.6%(446 名患者中的 132 名)。
这项队列研究中的主题模型聚类分析确定了 CLTI 中的 3 个不同阶段。研究结果表明,CLTI 无复发生存率是一个可以准确和可重复地量化的终点,并且可以用作以患者为中心的结局。
