Department of Obstetrics and Gynecology, Tokai University School of Medicine, Kanagawa, Japan.
Division of Gynecologic Oncology, Department of Obstetrics and Gynecology, University of Southern California, Los Angeles, CA, USA.
J Gynecol Oncol. 2022 May;33(3):e26. doi: 10.3802/jgo.2022.33.e26. Epub 2022 Feb 3.
To assess the efficacy of the FIGO 2018 classification system for nodal-specific classifications for early-stage cervical cancer; specifically, to examine the impact of nodal metastasis on survival and the effect of postoperative treatments, according to histological subtypes.
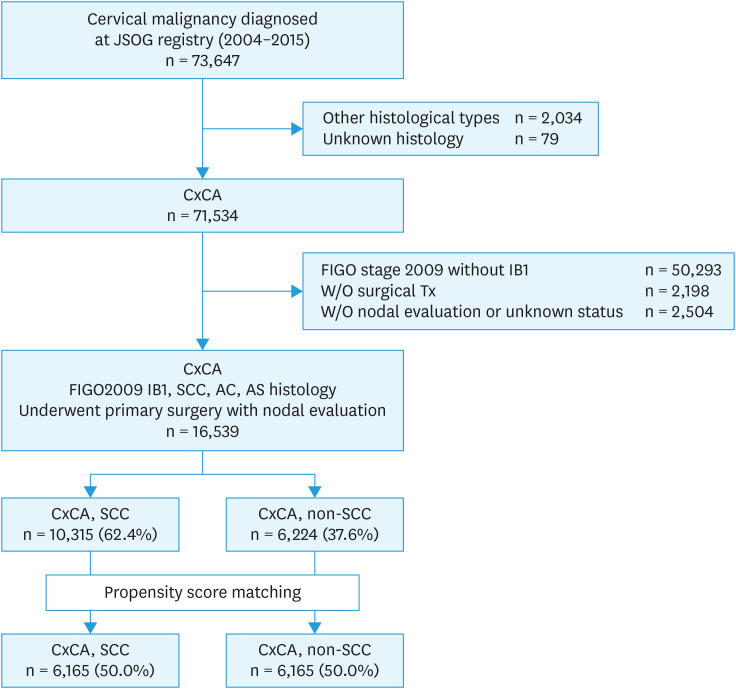
This society-based retrospective observational study in Japan examined 16,539 women with the 2009 FIGO stage IB1 cervical cancer who underwent primary surgical treatment from 2004 to 2015. Associations of cause-specific survival (CSS) with nodal metastasis and postoperative adjuvant therapy were examined according to histology type (squamous cell carcinoma [SCC], n=10,315; and non-SCC, n=6,224).
The nodal metastasis rate for SCC was higher than that for non-SCC (10.7% vs. 8.3%, p<0.001). In multivariable analysis, the impact of nodal metastasis on CSS was greater for non-SCC tumors (adjusted-hazard ratio [HR], 3.11; 95% confidence interval [CI], 2.40-4.02) than for SCC tumors (adjusted-HR, 2.20; 95% CI, 1.70-2.84; p<0.001). Propensity score matching analysis showed significantly lower CSS rates for women with pelvic nodal metastasis from non-SCC tumors than from SCC tumors (5-year CSS rate, 75.4% vs. 90.3%, p<0.001). The CSS rates for women with nodal metastasis in SCC histology were similar between the postoperative concurrent chemoradiotherapy/radiotherapy and chemotherapy groups (89.2% vs. 86.1%, p=0.42), whereas those in non-SCC histology who received postoperative chemotherapy improved the CSS (74.1% vs. 67.7%, p=0.043).
The node-specific staging system in the 2018 FIGO cervical cancer classification is applicable to both non-SCC tumors and SCC tumors; however, the prognostic significance of nodal metastases and efficacy of postoperative therapies vary according to histology.
评估 2018 年 FIGO 淋巴结特定分类系统在早期宫颈癌中的疗效;具体来说,根据组织学亚型,检查淋巴结转移对生存的影响以及术后治疗的效果。
本研究在日本进行了一项基于学会的回顾性观察研究,纳入了 16539 名 2009 年 FIGO 分期为 IB1 期的宫颈癌患者,这些患者均在 2004 年至 2015 年期间接受了初始手术治疗。根据组织学类型(鳞状细胞癌[SCC],n=10315;非 SCC,n=6224),检查了特定原因生存率(CSS)与淋巴结转移和术后辅助治疗的关系。
SCC 的淋巴结转移率高于非 SCC(10.7%比 8.3%,p<0.001)。多变量分析显示,淋巴结转移对非 SCC 肿瘤的 CSS 影响更大(调整后的危险比[HR],3.11;95%置信区间[CI],2.40-4.02),而对 SCC 肿瘤的影响较小(调整后 HR,2.20;95% CI,1.70-2.84;p<0.001)。倾向评分匹配分析显示,非 SCC 肿瘤的盆腔淋巴结转移患者的 CSS 率明显低于 SCC 肿瘤(5 年 CSS 率,75.4%比 90.3%,p<0.001)。SCC 组织学中淋巴结转移的患者,术后同步放化疗/放疗与化疗组的 CSS 率相似(89.2%比 86.1%,p=0.42),而非 SCC 组织学中接受术后化疗的患者 CSS 得到改善(74.1%比 67.7%,p=0.043)。
2018 年 FIGO 宫颈癌分类中的淋巴结特定分期系统适用于非 SCC 肿瘤和 SCC 肿瘤;然而,淋巴结转移的预后意义和术后治疗的效果根据组织学而有所不同。