Verma Anita, Vimalesvaran Sunitha, Dhawan Anil
Department of Infection Sciences, King's College Hospital, London SE5 9RS, UK.
Department of Paediatric Gastroenterology, Hepatology and Nutrition, King's College Hospital, London SE5 9RS, UK.
Antibiotics (Basel). 2022 Mar 15;11(3):387. doi: 10.3390/antibiotics11030387.
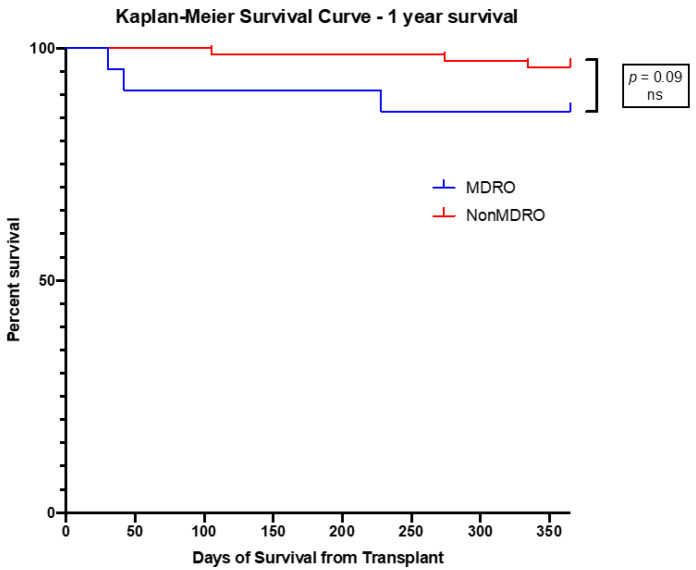
(1) Background: Multidrug-resistant organisms (MDRO) are a growing problem in liver transplant recipients (LTR), associated with high morbidity and mortality. We reviewed the impact of antimicrobial stewardship (AMS) and active screening of MDRO on the epidemiology and outcomes in paediatric LTR. (2) Methods: Single-centre retrospective review of paediatric LTR from January 2017 to December 2018. (3) Results: Ninety-six children were included; 32 (33%) patients were colonised with ≥1 MDRO and 22 (23%) patients had MDRO infections. Median (IQR) duration for start of infection was 9.5 (1.8−16.0) days. Colonisation rate with Gram-positive MDRO was 15.6%, with infection rate of 6.2%; majority due to Vancomycin-Resistant Enterococcus faecium (VRE). Colonisation with Gram-negative MDRO was 27.0%, with infection rate of 16.6%; majority due to extended-spectrum β-lactamase producing Enterobacteriaceae. Colonisation and infection rate due to Carbapenem-resistant Enterobacteriaceae was 6% and 3%, respectively, during screening and AMS, compared to historical control of 25% and 30%, respectively, without screening and AMS. There was significant reduction in VRE and CRE infection during AMS period in comparison to historical control. Pre-transplant risk factors including bacterial infections pre-transplant (p < 0.01), diagnosis of biliary atresia (p = 0.03), exposure to antibiotics (p < 0.01), EBV viraemia (p = 0.01), and auxiliary transplantation (p < 0.01) were associated with post-transplant MDRO infections. Patients with MDRO infections had longer length of hospital and paediatric intensive care unit stay days (p < 0.01) but associated with no mortality. (4) Conclusions: Our results demonstrate low incidence of colonisation and infections with MDRO, which were associated with high morbidity but no mortality in paediatric LTR. There was significant reduction in MRSA, VRE, and CRE during AMS period compared to pre-AMS era. Some risk factors are unavoidable but antibiotic overuse, early initiation of appropriate antibiotic therapy and effective infection prevention strategies can be monitored with multifaceted approach of AMS and screening of MDRO. With limited therapeutic options for MDRO and efficacy data of newer antibiotics in paediatric LTR, robust infection control practices are of paramount importance.
(1)背景:多重耐药菌(MDRO)在肝移植受者(LTR)中是一个日益严重的问题,与高发病率和死亡率相关。我们回顾了抗菌药物管理(AMS)和主动筛查MDRO对小儿肝移植受者的流行病学及预后的影响。(2)方法:对2017年1月至2018年12月的小儿肝移植受者进行单中心回顾性研究。(3)结果:纳入96名儿童;32名(33%)患者定植有≥1种MDRO,22名(23%)患者发生MDRO感染。感染开始的中位(四分位间距)持续时间为9.5(1.8−16.0)天。革兰氏阳性MDRO的定植率为15.6%,感染率为6.2%;大多数由耐万古霉素屎肠球菌(VRE)引起。革兰氏阴性MDRO的定植率为27.0%,感染率为16.6%;大多数由产超广谱β-内酰胺酶的肠杆菌科细菌引起。在筛查和AMS期间,耐碳青霉烯类肠杆菌科细菌的定植率和感染率分别为6%和3%,而在未进行筛查和AMS的历史对照中分别为25%和30%。与历史对照相比,AMS期间VRE和CRE感染显著减少。移植前的危险因素包括移植前细菌感染(p<0.01)、胆道闭锁诊断(p=0.03)、接触抗生素(p<0.01)、EBV病毒血症(p=0.01)和辅助移植(p<0.01)与移植后MDRO感染相关。发生MDRO感染的患者住院时间和儿科重症监护病房住院天数更长(p<0.01),但与死亡率无关。(4)结论:我们的结果表明,小儿肝移植受者中MDRO的定植和感染发生率较低,与高发病率相关,但无死亡率。与AMS前时代相比,AMS期间MRSA、VRE和CRE显著减少。一些危险因素不可避免,但抗生素的过度使用、适当抗生素治疗的早期启动以及有效的感染预防策略可以通过AMS和MDRO筛查的多方面方法进行监测。鉴于小儿肝移植受者中MDRO的治疗选择有限以及新型抗生素的疗效数据,强有力的感染控制措施至关重要。