Takeda Development Center Americas, Inc., Cambridge, MA, USA.
Department of Oncology Research and Early Development, Drug Metabolism and Pharmacokinetics, AstraZeneca, 35 Gatehouse Park, Waltham, MA, 02451, USA.
Eur J Drug Metab Pharmacokinet. 2022 Jul;47(4):467-482. doi: 10.1007/s13318-022-00763-y. Epub 2022 Mar 28.
Induction of drug-metabolizing enzymes can lead to drug-drug interactions (DDIs); therefore, early assessment is often conducted. Previous reports focused on true positive cytochrome P450 3A (CYP3A) inducers leaving a gap in translation for in vitro inducers which do not manifest in clinical induction. The goal herein was to expand the in vitro induction dataset by including true negative clinical inducers to identify a correction factor to basic DDI models, which reduces false positives without impacting false negatives.
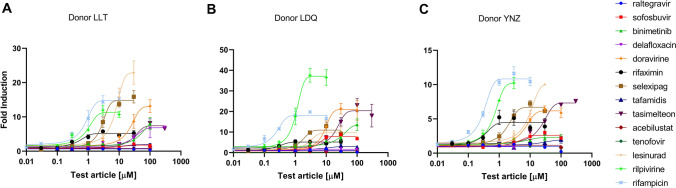
True negative clinical inducers were identified through a literature search, in vitro induction parameters were generated in three human hepatocyte donors, and the performance of basic induction models proposed by regulatory agencies, concentration producing twofold induction (F2), basic static model (R3) and relative induction score (RIS), was used to characterize clinical induction risk.
The data demonstrated the importance of correcting for in vitro binding and metabolism to derive induction parameters. The aggregate analysis indicates that the RIS with a positive cut-off of < 0.7-fold area under the curve ratio (AUCR) provides the best quantitative prediction. Additionally, correction factors of ten and two times the unbound peak plasma concentration at steady state (C) can be confidently used to identify true positive inducers when referenced against the concentration resulting in twofold increase in messenger ribonucleic acid (mRNA) or using the R3 equation, respectively.
These iterative improvements, which reduce the number of false positives, could aid regulatory recommendations and limit unnecessary clinical explorations into CYP3A induction.
诱导药物代谢酶可导致药物-药物相互作用(DDI);因此,通常会进行早期评估。先前的报告侧重于真正的细胞色素 P450 3A(CYP3A)诱导剂,而对于不会在临床诱导中表现出来的体外诱导剂,则存在翻译上的空白。本研究的目的是通过纳入真正的阴性临床诱导剂来扩展体外诱导数据集,以确定一种校正因子,从而减少对基础 DDI 模型的假阳性,而不影响假阴性。
通过文献检索确定真正的阴性临床诱导剂,在三位人类肝细胞供体中生成体外诱导参数,并使用监管机构提出的基本诱导模型,即浓度产生两倍诱导(F2)、基本静态模型(R3)和相对诱导评分(RIS),来评估临床诱导风险。
数据表明,校正体外结合和代谢以得出诱导参数非常重要。综合分析表明,RIS 的阳性截断值<0.7 倍曲线下面积比(AUCR)提供了最佳的定量预测。此外,当参考浓度导致信使核糖核酸(mRNA)增加两倍或使用 R3 方程时,分别使用稳态时未结合的峰血浆浓度(C)的 10 倍和 2 倍校正因子,可以有信心地识别真正的阳性诱导剂。
这些迭代改进可以减少假阳性的数量,有助于监管建议并限制对 CYP3A 诱导的不必要的临床探索。