Department of General, Visceral and Transplantation Surgery, Hannover Medical School, Carl-Neuberg Str. 1, 30625, Hannover, Germany.
Institute for Transfusion Medicine and Transplant Engineering, Hannover Medical School, Hannover, Germany.
World J Surg Oncol. 2022 Mar 30;20(1):100. doi: 10.1186/s12957-022-02559-5.
Recent studies focusing on thoracic surgery suggest postoperative kidney injury depending on the amount of perioperative blood transfusions. Data investigating similar effects after resection of colorectal liver metastases (CRLM) are not available. Aim of this study was therefore to evaluate the influence of perioperative blood transfusions on postoperative renal function and survival after resection of CRLM.
Seven hundred twenty-seven cases of liver resection for CRLM were retrospectively analyzed. Renal function was measured via estimated glomerular filtration rate (eGFR) and a postoperative decline of ≥ 10% was considered substantial. Potential influences on postoperative kidney function were assessed using univariable and multivariable logistic regression analyses. Cox-regression analyses were performed to estimate the impact on overall survival (OS).
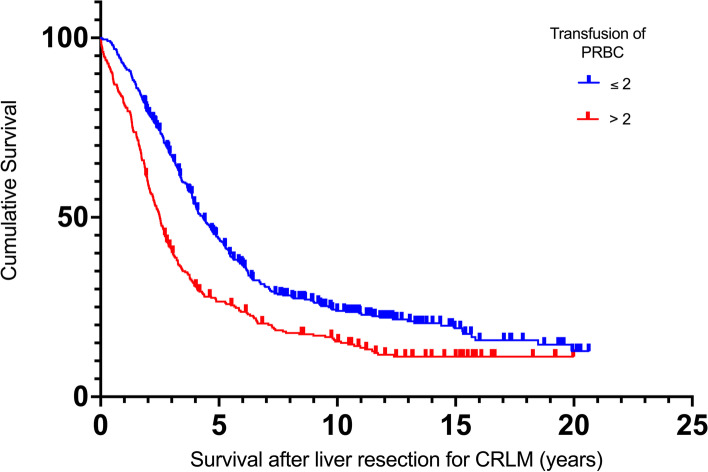
Preoperative impaired kidney function (p = 0.001, OR 2.477) and transfusion of > 2 units of packed red blood cells (PRBC) (p = 0.046; OR 1.638) were independently associated with an increased risk for ≥ 10% loss of renal function. Neither a pre-existing renal impairment, nor the additional loss of renal function were associated with reduced survival. Chemotherapies in the context of primary colorectal cancer treatment (p = 0.002), age > 70 years at liver resection (p = 0.005), number (p = 0.001), and size of metastases > 50 mm (p = 0.018), duration of resection > 120 min (p = 0.006) and transfusions of > 2 units of PRBC (p = 0.039) showed a negative independent influence on OS.
The results demonstrate a negative impact of perioperative blood transfusions on the postoperative renal function and OS. Hence, efforts to reduce blood transfusions should be intensified.
最近的胸部外科研究表明,术后肾脏损伤取决于围手术期的输血量。目前尚无研究调查结直肠癌肝转移(CRLM)切除术后类似影响的数据。因此,本研究旨在评估围手术期输血对 CRLM 切除术后肾功能和生存的影响。
回顾性分析了 727 例 CRLM 肝切除术病例。通过估算肾小球滤过率(eGFR)测量肾功能,术后下降≥10%被认为是显著的。使用单变量和多变量逻辑回归分析评估对术后肾功能的潜在影响。Cox 回归分析用于估计对总生存(OS)的影响。
术前肾功能受损(p=0.001,OR 2.477)和输血>2 单位浓缩红细胞(p=0.046;OR 1.638)与≥10%肾功能丧失的风险增加独立相关。预先存在的肾功能损害或肾功能的额外丧失与生存时间缩短无关。原发性结直肠癌治疗中的化疗(p=0.002)、肝切除时年龄>70 岁(p=0.005)、肝转移的数量(p=0.001)和大小>50mm(p=0.018)、手术时间>120 分钟(p=0.006)和输血>2 单位浓缩红细胞(p=0.039)均对 OS 有负面影响。
这些结果表明围手术期输血对术后肾功能和 OS 有负面影响。因此,应加强减少输血的努力。