Wu Yan, Pu Cailing, Zhu Wenchao, He Chengbin, Fei Jingle, Hu Hongjie
Department of Radiology, Sir Run Run Shaw Hospital, Zhejiang University School of Medicine, Hangzhou, China.
Department of Radiology, Lishui Central Hospital, Lishui, China.
Front Cardiovasc Med. 2022 Mar 9;9:817456. doi: 10.3389/fcvm.2022.817456. eCollection 2022.
Cardiac light-chain amyloidosis (AL CA) portends poor prognosis. Contrast cardiac magnetic resonance (CMR) with late gadolinium enhancement (LGE) imaging is an important tool in recognizing AL CA. But contraindications to contrast CMR would significantly restrict its clinical application value. Our study aims to construct a convenient risk score to help identify cardiac involvement in patients at risk of AL CA. Moreover, we also investigate whether this risk score could provide prognosis information.
Sixty-three patients at risk of AL CA were retrospectively included in our study. Basic clinical characters, lab results, 12-lead electrocardiogram data, and cardiac magnetic resonance image data were collected. AL CA was diagnosed according to typical CA LGE pattern. Logistic analysis was used to figure out predictive parameters of AL CA and their β coefficients, further constructing the risk score. Receiver operating characteristics (ROC) curve was used to find the cut-off point best distinguishing AL CA+ from AL CA-patients. Bootstrapping was used for internal validation. All patients were divided into high-risk and low-risk group according to the diagnostic cut-off point, and followed up for survival information. Kaplan-Meier plots and log-rank test were performed to analyze if this score had prognostic value.
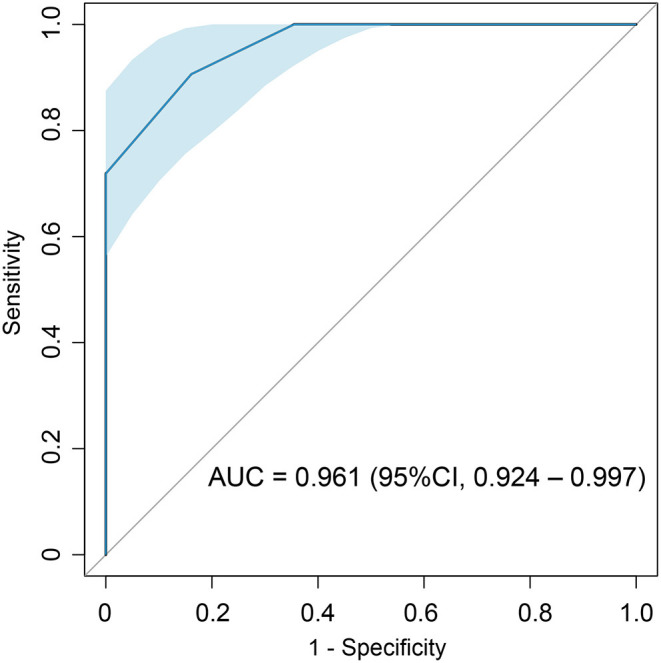
The risk score finally consisted of 4 parameters: pericardial effusion (PE) (1 point), low electrocardiographic QRS voltages (LQRSV) (1 point), CMR-derived impaired global radial strain (GRS) (<15.14%) (1 point) and increased left ventricular maximum wall thickness (LVMWT) (>13 mm) (2 points). Total score ranged from 0 to 5 points. A cut-off point of 1.5 showed highest accuracy in diagnosing AL CA with an AUC of 0.961 (95% CI: 0.924-0.997, sensitivity: 90.6%, specificity: 83.9%). Kaplan-Meier plots and log-rank test showed that the high-risk group had significantly poor overall survival rates.
In patients at risk of AL CA, a risk score incorporating the presence of PE, LQRSV, and CMR-derived impaired GRS and increased LVMWT is predictive of a diagnosis of AL CA by LGE criteria. This risk score may be helpful especially when contrast CMR is not available or contraindicated, and further studies should be considered to validate this score.
心脏轻链淀粉样变(AL CA)预后较差。钆剂延迟增强(LGE)成像的对比增强心脏磁共振(CMR)是识别AL CA的重要工具。但对比增强CMR的禁忌症会显著限制其临床应用价值。我们的研究旨在构建一个便捷的风险评分,以帮助识别有AL CA风险的患者的心脏受累情况。此外,我们还研究了这个风险评分是否能提供预后信息。
本研究回顾性纳入了63例有AL CA风险的患者。收集基本临床特征、实验室检查结果、12导联心电图数据和心脏磁共振图像数据。根据典型的CA LGE模式诊断AL CA。采用逻辑分析确定AL CA的预测参数及其β系数,进一步构建风险评分。采用受试者工作特征(ROC)曲线确定区分AL CA阳性和阴性患者的最佳切点。采用自抽样法进行内部验证。根据诊断切点将所有患者分为高危组和低危组,并随访生存信息。采用Kaplan-Meier曲线和对数秩检验分析该评分是否具有预后价值。
风险评分最终由4个参数组成:心包积液(PE)(1分)、心电图QRS波低电压(LQRSV)(1分)、CMR衍生的整体径向应变受损(GRS)(<15.14%)(1分)和左心室最大壁厚增加(LVMWT)(>13 mm)(2分)。总分范围为0至5分。切点为1.5时,诊断AL CA的准确性最高,AUC为0.961(95%CI:0.924-0.997,敏感性:90.6%,特异性:83.9%)。Kaplan-Meier曲线和对数秩检验显示,高危组的总生存率显著较差。
在有AL CA风险的患者中,结合PE、LQRSV、CMR衍生的GRS受损和LVMWT增加的风险评分可预测LGE标准下的AL CA诊断。该风险评分可能特别有助于在无法进行或禁忌对比增强CMR的情况下,应考虑进一步研究以验证该评分。