Gomes Nayana F A, Silva Vicente Rezende, Levine Robert A, Esteves William A M, de Castro Marildes Luiza, Passos Livia S A, Dal-Bianco Jacob P, Pantaleão Alexandre Negrão, da Silva Jose Luiz Padilha, Tan Timothy C, Dutra Walderez O, Aikawa Elena, Hung Judy, Nunes Maria Carmo P
School of Medicine, Hospital das Clínicas, Federal University of Minas Gerais, Belo Horizonte, Brazil.
Cardiac Ultrasound Lab, Harvard Medical School, Massachusetts General Hospital, Boston, MA, United States.
Front Cardiovasc Med. 2022 Mar 11;9:862382. doi: 10.3389/fcvm.2022.862382. eCollection 2022.
Mitral regurgitation (MR) is the most common valve abnormality in rheumatic heart disease (RHD) often associated with stenosis. Although the mechanism by which MR develops in RHD is primary, longstanding volume overload with left atrial (LA) remodeling may trigger the development of secondary MR, which can impact on the overall progression of MR. This study is aimed to assess the incidence and predictors of MR progression in patients with RHD.
Consecutive RHD patients with non-severe MR associated with any degree of mitral stenosis were selected. The primary endpoint was a progression of MR, which was defined as an increase of one grade in MR severity from baseline to the last follow-up echocardiogram. The risk of MR progression was estimated accounting for competing risks.
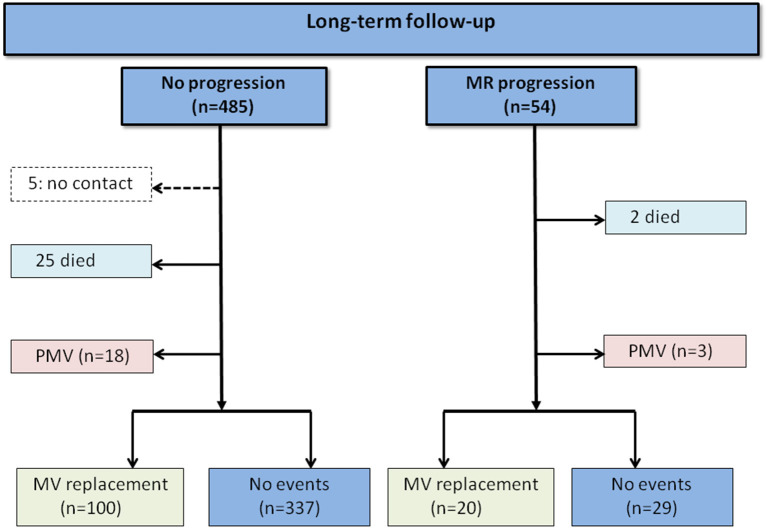
The study included 539 patients, age of 46.2 ± 12 years and 83% were women. At a mean follow-up time of 4.2 years (interquartile range [IQR]: 1.2-6.9 years), 54 patients (10%) displayed MR progression with an overall incidence of 2.4 per 100 patient-years. Predictors of MR progression by the Cox model were age (adjusted hazard ratio [HR] 1.541, 95% CI 1.222-1.944), and LA volume (HR 1.137, 95% CI 1.054-1.226). By considering competing risk analysis, the direction of the association was similar for the rate (Cox model) and incidence (Fine-Gray model) of MR progression. In the model with LA volume, atrial fibrillation (AF) was no longer a predictor of MR progression. In the subgroup of patients in sinus rhythm, 59 had an onset of AF during follow-up, which was associated with progression of MR (HR 2.682; 95% CI 1.133-6.350).
In RHD patients with a full spectrum of MR severity, progression of MR occurs over time is predicted by age and LA volume. LA enlargement may play a role in the link between primary MR and secondary MR in patients with RHD.
二尖瓣反流(MR)是风湿性心脏病(RHD)中最常见的瓣膜异常,常与狭窄相关。虽然RHD中MR发生的机制是原发性的,但长期容量超负荷伴左心房(LA)重塑可能引发继发性MR的发展,这可能影响MR的整体进展。本研究旨在评估RHD患者中MR进展的发生率和预测因素。
选取连续的伴有任何程度二尖瓣狭窄的非重度MR的RHD患者。主要终点是MR进展,定义为从基线到最后一次随访超声心动图时MR严重程度增加一级。考虑竞争风险来估计MR进展的风险。
该研究纳入了539例患者,年龄为46.2±12岁,83%为女性。平均随访时间为4.2年(四分位间距[IQR]:1.2 - 6.9年),54例患者(10%)出现MR进展,总发生率为每100患者年2.4例。Cox模型中MR进展的预测因素为年龄(调整后风险比[HR] 1.541,95%可信区间[CI] 1.222 - 1.944)和LA容积(HR 1.137,95% CI 1.054 - 1.226)。通过竞争风险分析,MR进展的发生率(Cox模型)和发病率(Fine - Gray模型)的关联方向相似。在包含LA容积的模型中,心房颤动(AF)不再是MR进展的预测因素。在窦性心律患者亚组中,59例在随访期间发生AF,这与MR进展相关(HR 2.682;95% CI 1.133 - 6.350)。
在具有各种MR严重程度的RHD患者中,MR进展随时间发生,其可由年龄和LA容积预测。LA增大可能在RHD患者原发性MR和继发性MR之间的关联中起作用。