Winant Abbey J, Callahan Ryan, Vargas Sara O, Jenkins Kathy J, Rameh Vanessa, Johnston Patrick R, Niccum Maria, Keochakian Mirjam L, Lee Edward Y
Department of Radiology, Boston Children's Hospital, Harvard Medical School, 300 Longwood Avenue, Boston, MA 02115, USA.
Department of Cardiology, Boston Children's Hospital, Harvard Medical School, 300 Longwood Avenue, Boston, MA 02115, USA.
Children (Basel). 2022 Apr 12;9(4):543. doi: 10.3390/children9040543.
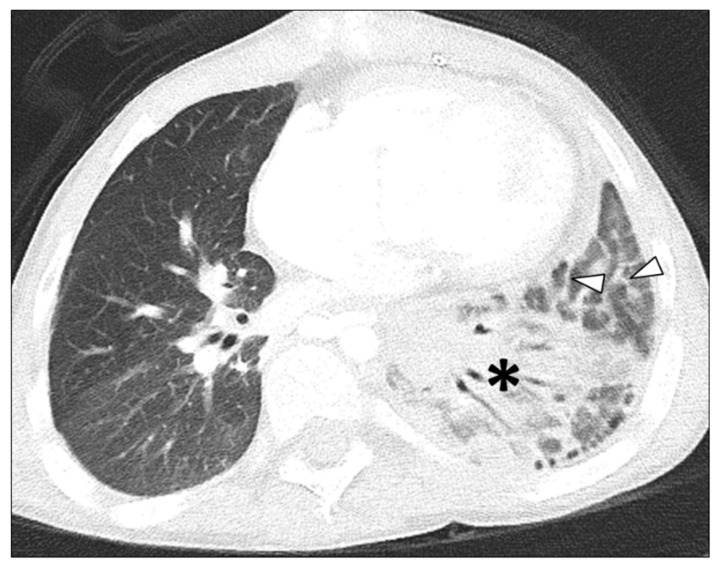
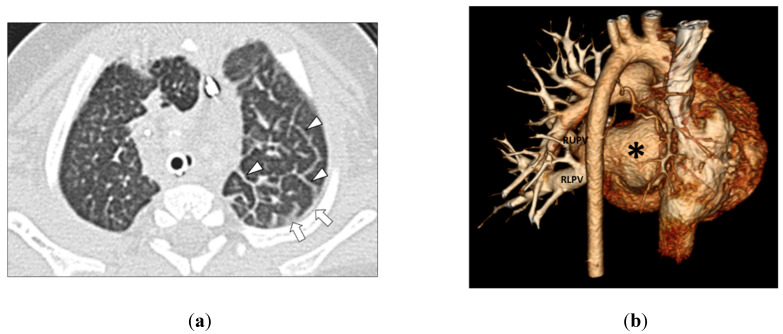
Purpose: To retrospectively compare the lung and pleural findings in children with pulmonary vein stenosis (PVS) with and without aspiration on multidetector computed tomography (MDCT). Materials and Methods: All consecutive children (≤18 years old) with PVS who underwent thoracic MDCT studies from August 2004 to December 2021 were categorized into two groups: children with PVS with aspiration (Group 1) and children with PVS without aspiration (Group 2). Two independent pediatric radiologists retrospectively evaluated thoracic MDCT studies for the presence of lung and pleural abnormalities as follows: (1) in the lung (ground-glass opacity (GGO), consolidation, nodule, mass, cyst(s), interlobular septal thickening, and fibrosis) and (2) in the pleura (thickening, effusion, and pneumothorax). Interobserver agreement between the two reviewers was evaluated by the proportion of agreement and the Kappa statistic. Results: The final study population consisted of 64 pediatric patients (36 males (56.3%) and 43 females (43.7%); mean age, 1.7 years; range, 1 day−17 years). Among these 64 patients, 19 patients (29.7%) comprised Group 1 and the remaining 45 patients (70.3%) comprised Group 2. In Group 1 (children with PVS with aspiration), the detected lung and pleural MDCT abnormalities were: GGO (17/19; 89.5%), pleural thickening (17/19; 89.5%), consolidation (16/19; 84.5%), and septal thickening (16/19; 84.5%). The lung and pleural MDCT abnormalities observed in Group 2 (children with PVS without aspiration) were: GGO (37/45; 82.2%), pleural thickening (37/45; 82.2%), septal thickening (36/45; 80%), consolidation (3/45; 6.7%), pleural effusion (1/45; 2.2%), pneumothorax (1/45; 2.2%), and cyst(s) (1/45; 2.2%). Consolidation was significantly more common in pediatric patients with both PVS and aspiration (Group 1) (p < 0.001). There was high interobserver agreement between the two independent reviewers for detecting lung and pleural abnormalities on thoracic MDCT studies (Kappa = 0.98; CI = 0.958, 0.992). Conclusion: Aspiration is common in pediatric patients with PVS who undergo MDCT and was present in nearly 30% of all children with PVS during our study period. Consolidation is not a typical radiologic finding of PVS in children without clinical evidence of aspiration. When consolidation is present on thoracic MDCT studies in pediatric patients with PVS, the additional diagnosis of concomitant aspiration should be considered.
回顾性比较多层螺旋计算机断层扫描(MDCT)检查中,有吸入史和无吸入史的小儿肺静脉狭窄(PVS)患者的肺部和胸膜表现。材料与方法:将2004年8月至2021年12月期间接受胸部MDCT检查的所有连续PVS患儿(≤18岁)分为两组:有吸入史的PVS患儿(第1组)和无吸入史的PVS患儿(第2组)。两名独立的儿科放射科医生回顾性评估胸部MDCT检查结果,以确定肺部和胸膜异常情况,如下:(1)肺部(磨玻璃影(GGO)、实变、结节、肿块、囊肿、小叶间隔增厚和纤维化);(2)胸膜(增厚、积液和气胸)。通过一致性比例和Kappa统计量评估两位阅片者之间的观察者间一致性。结果:最终研究人群包括64例儿科患者(36例男性(56.3%)和43例女性(43.7%);平均年龄1.7岁;范围1天至17岁)。在这64例患者中,19例患者(29.7%)属于第1组,其余45例患者(70.3%)属于第2组。在第1组(有吸入史的PVS患儿)中,MDCT检测到的肺部和胸膜异常包括:GGO(17/19;89.5%)、胸膜增厚(17/19;89.5%)、实变(16/19;84.5%)和小叶间隔增厚(16/19;84.5%)。在第2组(无吸入史的PVS患儿)中观察到的肺部和胸膜MDCT异常包括:GGO(37/45;82.2%)、胸膜增厚(37/45;82.2%)、小叶间隔增厚(36/45;80%)、实变(3/45;6.7%)、胸腔积液(1/45;2.2%)、气胸(1/45;2.2%)和囊肿(1/45;2.2%)。实变在同时患有PVS和有吸入史的儿科患者(第1组)中明显更常见(p < 0.001)。两位独立阅片者在胸部MDCT检查中检测肺部和胸膜异常方面具有高度的观察者间一致性(Kappa = 0.98;CI = 0.958,0.99)。结论:在接受MDCT检查的PVS儿科患者中,吸入情况很常见,在我们的研究期间,近30%的PVS患儿存在吸入。在没有临床吸入证据的儿童中,实变不是PVS的典型影像学表现。当PVS儿科患者的胸部MDCT检查出现实变时,应考虑同时存在吸入的额外诊断。