Department of Cardiovascular Surgery, Nerima Hospital, Juntendo University, 3-1-10, Takanodai, Nerima-ku, Tokyo, 177-8521, Japan.
Department of Cardiovascular Surgery, Juntendo University, Bunkyo-Ku, Tokyo, Japan.
J Cardiothorac Surg. 2022 Apr 27;17(1):83. doi: 10.1186/s13019-022-01827-5.
Pseudoaneurysm with a shunt to the right ventricle after aortic repair for acute aortic dissection is an extremely rare and life-threatening condition. Surgical treatment is unavoidable, but surgery is complicated, and there are some pitfalls. This study describes the reoperation performed in a patient at a high surgical risk by clarifying the shunt site using multimodality imaging before surgery.
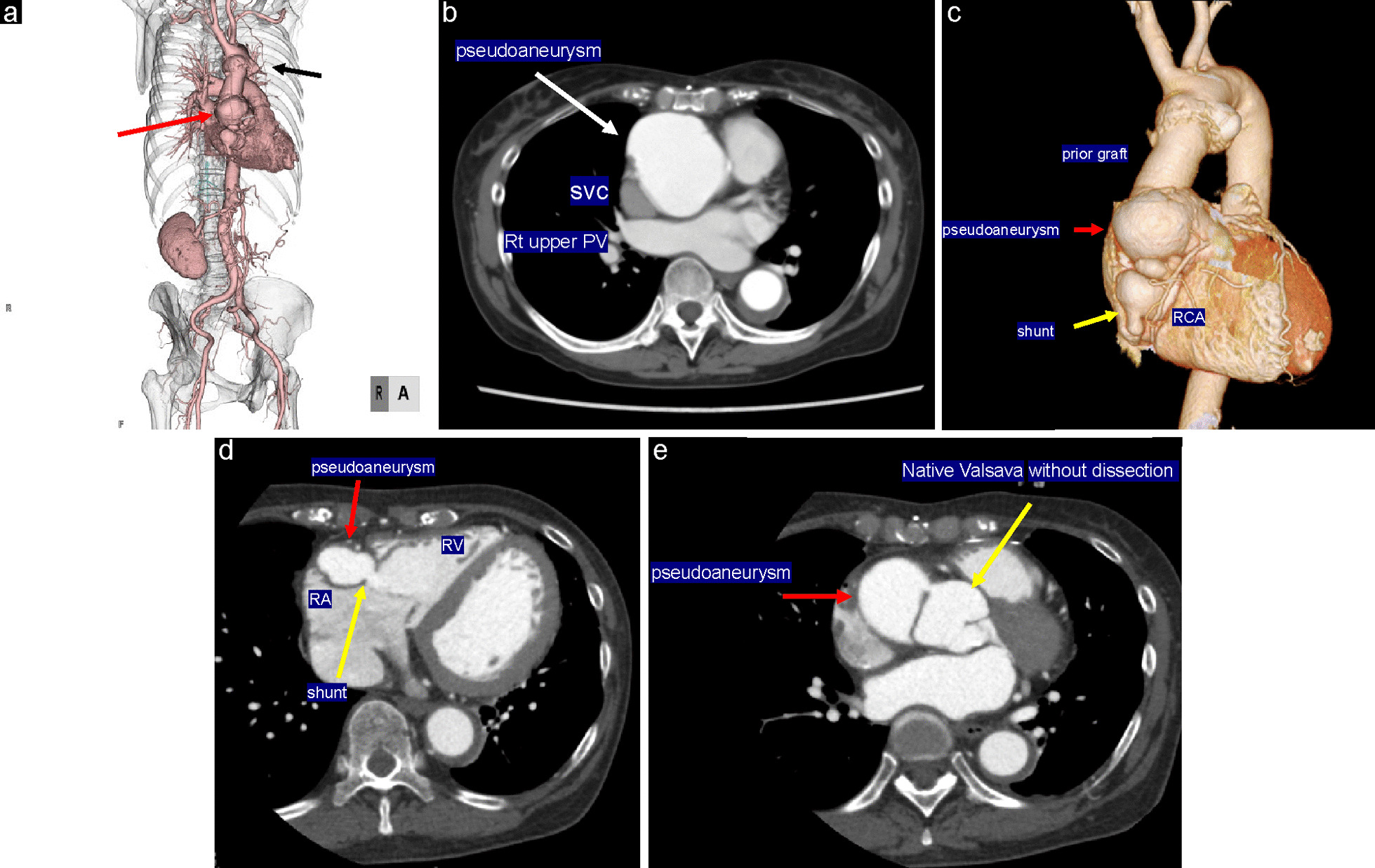
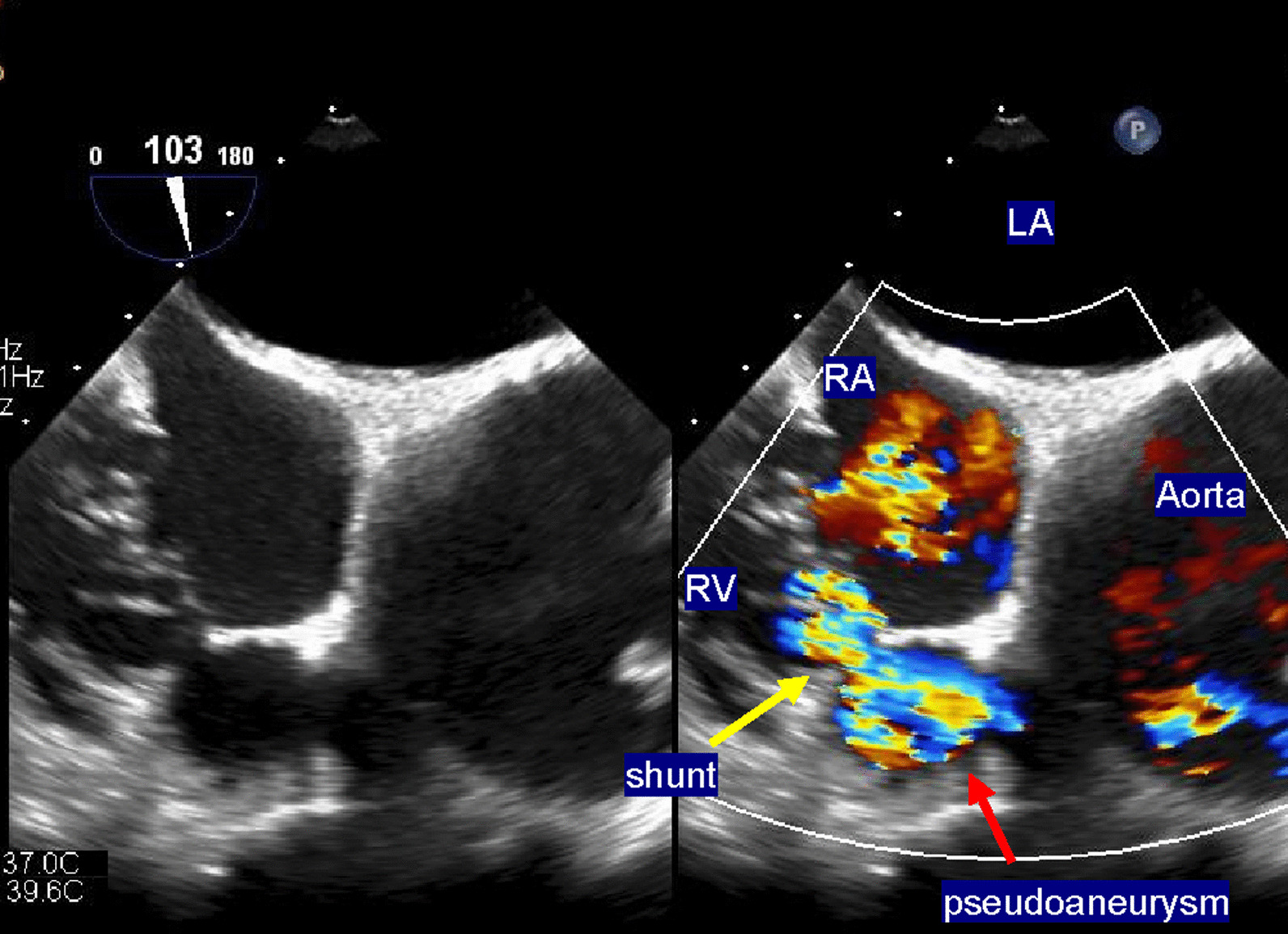
A 69-year-old woman with a history of systemic lupus erythematosus (SLE) and Sjogren's syndrome presented with a pseudoaneurysm 1 year after emergency surgery for acute type A aortic dissection. Eight years after the first surgery, she experienced sudden chest pain and presented to the emergency department. Her dyspnea worsened; therefore, echocardiography and three-dimensional computed tomography (3DCT) were performed, and a pseudoaneurysm and shunt to the right ventricle were identified. The medical team attempted to close the shunt with a percutaneous catheter but was unsuccessful, and she was referred to our department for surgical treatment. The pseudoaneurysm originating from the proximal side of the aorta was large (diameter = 55 mm), and echocardiography-gated 3DCT identified the shunt from the pseudoaneurysm to the right ventricle. First, extracorporeal circulation was initiated, and resternotomy was performed. We could not insert the left ventricular venting tube from the right side because of the pseudoaneurysm size. Instead, the tube was inserted from the left atrial appendage. We found a half-circumferential disengaged anastomosis around the proximal anastomosis, which formed the large pseudoaneurysm leading to a fistula in the right ventricle. We closed the fistula and performed a Bentall operation. The patient had a good postoperative course and was discharged on postoperative day 21. She continued treatment for SLE and Sjogren's syndrome, and her inflammatory reaction improved.
We performed a Bentall operation and fistula closure with resternotomy in a patient with type A aortic dissection with SLE and Sjogren's syndrome. Multimodal imaging is essential in defining the pseudoaneurysm and the fistula surrounding the anatomy while ensuring their resolution and guiding the approach for operation.
急性主动脉夹层修复术后出现通往右心室的假性动脉瘤是一种极其罕见且危及生命的情况。手术治疗是不可避免的,但手术复杂,存在一些陷阱。本研究通过在手术前使用多模态成像明确分流部位,描述了一位高手术风险患者的再次手术。
一位 69 岁女性,有系统性红斑狼疮(SLE)和干燥综合征(Sjogren 综合征)病史,在急性 A 型主动脉夹层的急诊手术后 1 年出现假性动脉瘤。第一次手术后 8 年,她突发胸痛并到急诊科就诊。她的呼吸困难加重;因此,进行了超声心动图和三维计算机断层扫描(3DCT),发现假性动脉瘤和通往右心室的分流。医疗团队试图用经皮导管关闭分流,但未成功,随后转诊到我科进行手术治疗。源于主动脉近端的假性动脉瘤较大(直径=55mm),超声心动图门控 3DCT 显示假性动脉瘤与右心室之间的分流。首先,启动体外循环,并进行胸骨切开术。由于假性动脉瘤的大小,我们无法从右侧插入左心室引流管。相反,该管从左心耳插入。我们发现近端吻合口周围有半圆周分离吻合,形成通往右心室的大假性动脉瘤,并形成瘘管。我们关闭瘘管并进行 Bentall 手术。患者术后恢复良好,于术后第 21 天出院。她继续接受 SLE 和干燥综合征的治疗,炎症反应得到改善。
我们对患有 SLE 和干燥综合征的 A 型主动脉夹层患者进行了胸骨切开术的 Bentall 手术和瘘管闭合术。多模态成像对于明确假性动脉瘤和周围解剖结构的瘘管至关重要,同时确保其解决并指导手术方法。