Lee Seon-Hwa, Cho Iksung, You Seng-Chan, Cha Min-Jae, Chang Jee-Suk, Kim William D, Go Kyu-Yong, Kim Dae-Young, Seo Jiwon, Shim Chi-Young, Hong Geu-Ru, Kang Seok-Min, Ha Jong-Won, Rha Sun-Young, Kim Hyo-Song
Division of Cardiology, Severance Cardiovascular Hospital, Yonsei University College of Medicine, Seoul 03722, Korea.
Department of Biomedical Systems Informatics, Yonsei University College of Medicine, Seoul 03722, Korea.
Cancers (Basel). 2022 May 7;14(9):2320. doi: 10.3390/cancers14092320.
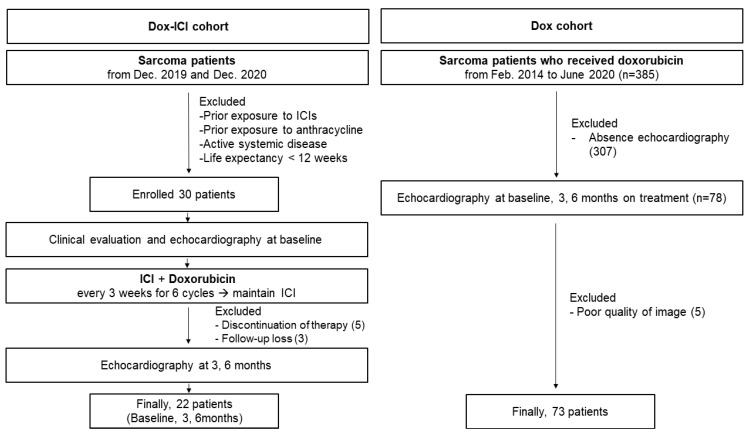
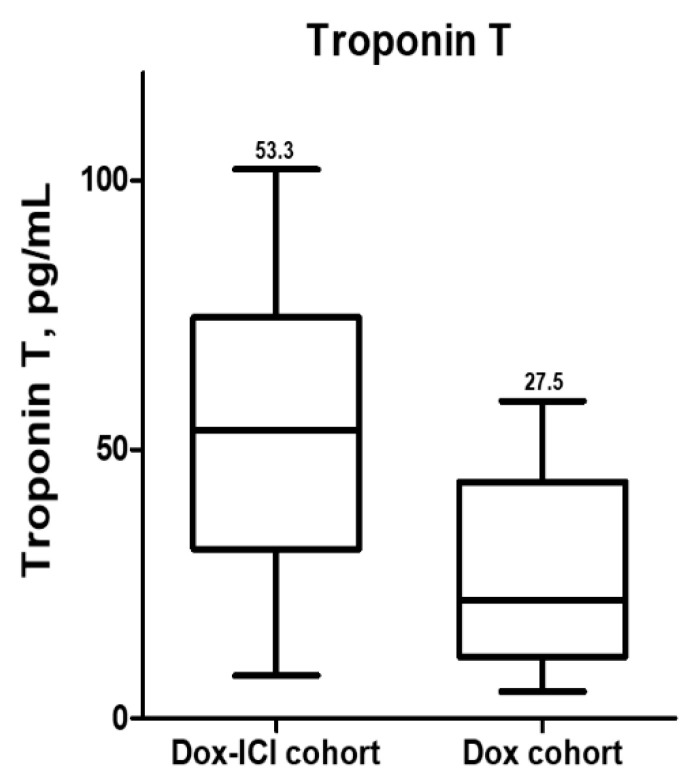
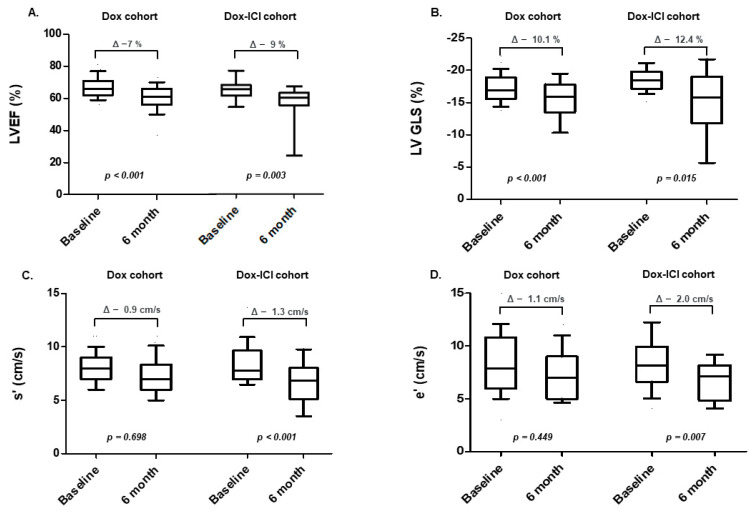
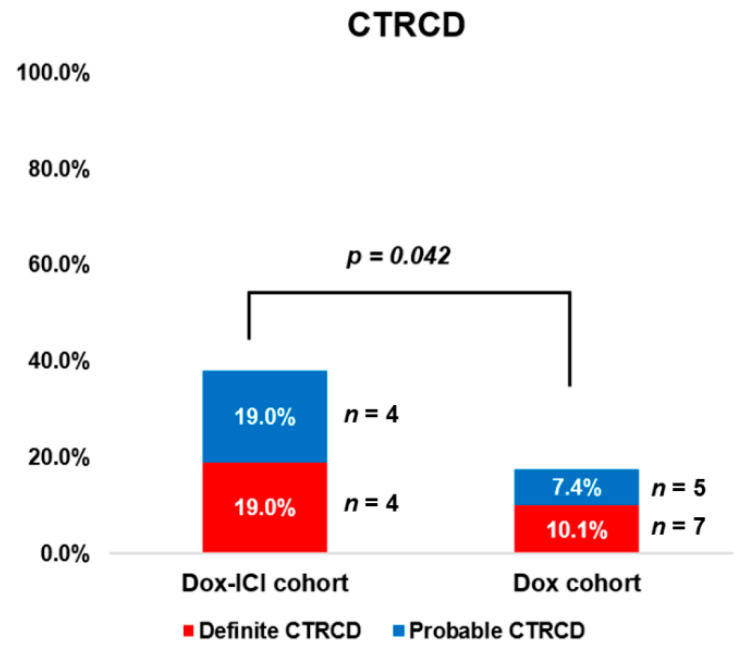
Backgrounds: There are scarce data on whether immune checkpoint inhibitors (ICIs) increase the risk of cardiac dysfunction when used with cardiotoxic agents. Thus, we evaluated cardiac dysfunction in patients with sarcoma receiving doxorubicin with or without ICI using echocardiography and left ventricular global longitudinal strain (LVGLS). Methods: A total of 95 patients were included in this study. Echocardiography and LVGLS were evaluated at baseline and follow-up (at 3 and 6 months of chemotherapy) and compared with the doxorubicin (Dox; n = 73) and concomitant ICI with doxorubicin (Dox-ICI; n = 22) groups. Cancer therapy-related cardiac dysfunction (CTRCD) was defined as a left ventricular ejection fraction (LVEF) drop of >10% and LVEF of <50% (definite CTRCD), LVEF drop of >10%, LVEF of ≥50%, and LVGLS relative reduction of >15% (probable CTRCD) at six months. Results: There were no significant differences in age, cumulative dose of doxorubicin, and cardiovascular risk factors between the two groups. At baseline, the LVEF was similar in the Dox and Dox-ICI groups (p = 0.493). In the Dox group, LVEF decreased to 59 ± 6% (Δ −7 ± 1.3%, p < 0.001) and LVGLS decreased from −17.3 ± 3.2% to −15.4 ± 3.2% (Δ −10.1 ± −1.9%, p < 0.001) at six months. In the Dox-ICI group, LVEF decreased to 55 ± 9% (Δ −9 ± 2.1%, p < 0.001), along with a significant decrease in LVGLS (from −18.6 ± 1.9% to −15.3 ± 3.6%, Δ −12.4 ± −2.4%, p < 0.001). Over a median follow-up of 192 days, there were no cases with clinical manifestations of fulminant myocarditis. In the Dox group, definite and probable CTRCD were observed in seven (10.1%) and five (7.4%) patients, respectively. In the Dox-ICI group, definite and probable CTRCD were observed in four (19%) and four (19%) patients, respectively. The total number of patients who developed CTRCD was significantly higher in the Dox-ICI group than in the Dox group (38.1% vs. 17.4%, p = 0.042). Serum troponin-T level was significantly higher in the Dox-ICI group than in the Dox group (53.3 vs. 27.5 pg/mL, p = 0.023). Conclusions: ICIs may increase the risk of CTRCD when used with cardiotoxic agents. CTRCD should be monitored in patients treated with ICIs by cardiac biomarkers and echocardiography, including LV-GLS.
关于免疫检查点抑制剂(ICI)与心脏毒性药物联用时是否会增加心脏功能障碍风险的数据稀缺。因此,我们使用超声心动图和左心室整体纵向应变(LVGLS)评估了接受多柔比星治疗的肉瘤患者在使用或不使用ICI时的心脏功能障碍情况。方法:本研究共纳入95例患者。在基线期以及随访期(化疗3个月和6个月时)评估超声心动图和LVGLS,并将其与多柔比星组(n = 73)和多柔比星联合ICI组(Dox-ICI;n = 22)进行比较。癌症治疗相关心脏功能障碍(CTRCD)定义为六个月时左心室射血分数(LVEF)下降>10%且LVEF<50%(明确的CTRCD),LVEF下降>10%,LVEF≥50%,且LVGLS相对降低>15%(可能的CTRCD)。结果:两组患者在年龄、多柔比星累积剂量和心血管危险因素方面无显著差异。基线时,多柔比星组和Dox-ICI组的LVEF相似(p = 0.493)。在多柔比星组中,六个月时LVEF降至59±6%(Δ -7±1.3%,p<0.001),LVGLS从-17.3±3.2%降至-15.4±3.2%(Δ -10.1±-1.9%,p<0.001)。在Dox-ICI组中,LVEF降至55±9%(Δ -9±2.1%,p<0.001),同时LVGLS显著降低(从-18.6±1.9%降至-15.3±3.6%,Δ -12.4±-2.4%,p<0.001)。在中位随访192天期间,未出现暴发性心肌炎临床表现的病例。在多柔比星组中,分别有7例(10.1%)和5例(7.4%)患者出现明确和可能的CTRCD。在Dox-ICI组中,分别有4例(19%)和4例(19%)患者出现明确和可能的CTRCD。发生CTRCD的患者总数在Dox-ICI组显著高于多柔比星组(38.1%对17.4%,p = 0.042)。Dox-ICI组血清肌钙蛋白-T水平显著高于多柔比星组(53.3对27.5 pg/mL,p = 0.023)。结论:ICI与心脏毒性药物联用时可能会增加CTRCD风险。对于接受ICI治疗的患者,应通过心脏生物标志物和超声心动图(包括LV-GLS)监测CTRCD。