Jahn Nora, Voelker Maria Theresa, Laudi Sven, Stehr Sebastian, Schneeberger Stefan, Brandacher Gerald, Sucher Elisabeth, Rademacher Sebastian, Seehofer Daniel, Sucher Robert, Hau Hans Michael
Department of Anesthesiology and Intensive Care Medicine, University Hospital of Leipzig, 04103 Leipzig, Germany.
Department of Visceral, Transplant and Thoracic Surgery, Innsbruck Medical University, 6020 Innsbruck, Austria.
J Clin Med. 2022 May 3;11(9):2563. doi: 10.3390/jcm11092563.
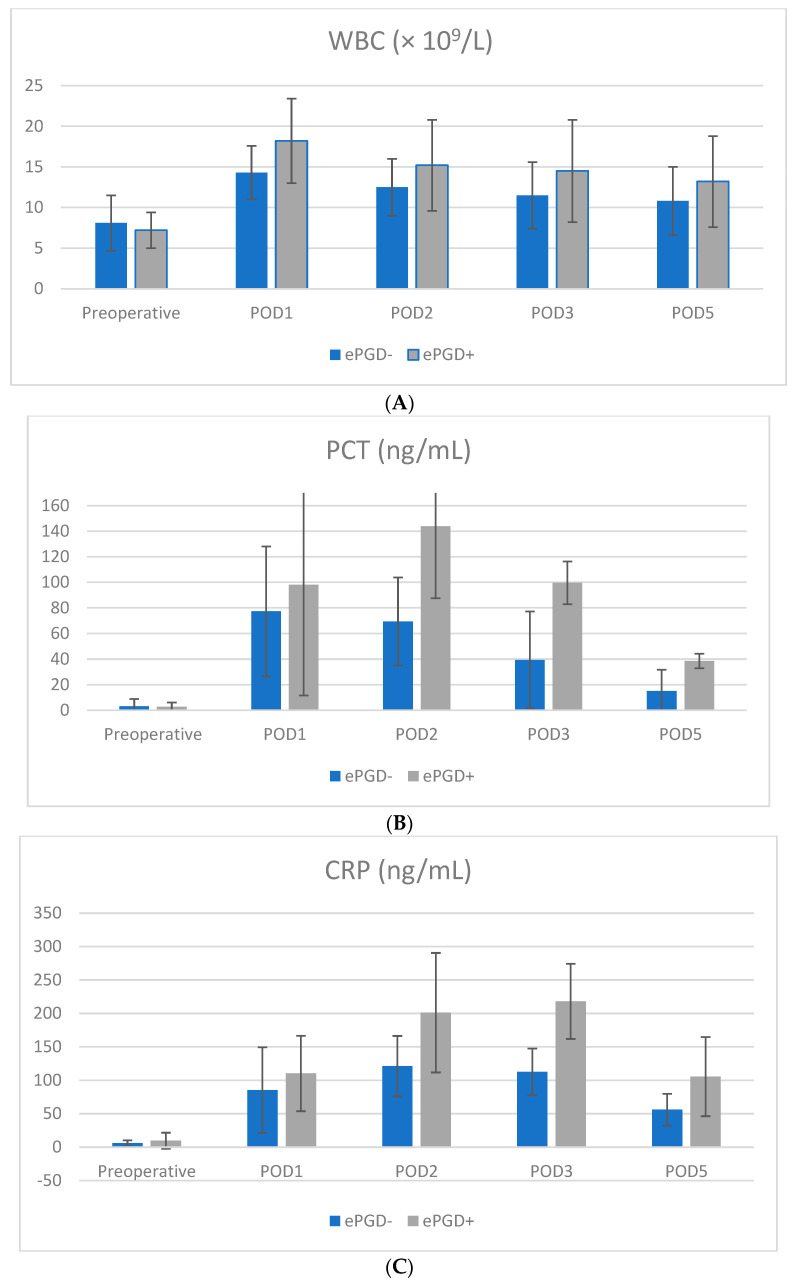
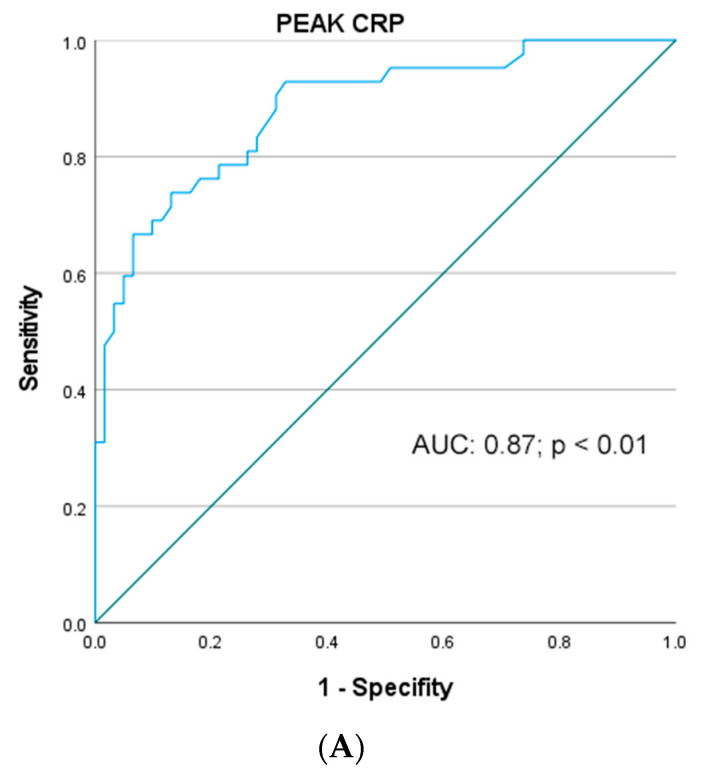
Background: Despite recent advances and refinements in perioperative management of simultaneous pancreas−kidney transplantation (SPKT) early pancreatic graft dysfunction (ePGD) remains a critical problem with serious impairment of early and long-term graft function and outcome. Hence, we evaluated a panel of classical blood serum markers for their value in predicting early graft dysfunction in patients undergoing SPKT. Methods: From a prospectively collected database medical data of 105 patients undergoing SPKT between 1998 and 2018 at our center were retrospectively analyzed. The primary study outcome was the detection of occurrence of early pancreatic graft dysfunction (ePGD), the secondary study outcome was early renal graft dysfunction (eRGD) as well as all other outcome parameters associated with the graft function. In this context, ePGD was defined as pancreas graft-related complications including graft pancreatitis, pancreatic abscess/peritonitis, delayed graft function, graft thrombosis, bleeding, rejection and the consecutive need for re-laparotomy due to graft-related complications within 3 months. With regard to analyzing ePGD, serum levels of white blood cell count (WBC), C-reactive protein (CRP), procalcitonin (PCT), pancreatic lipase as well as neutrophil−lymphocyte ratio (NLR) and platelet−lymphocyte ratio (PLR) were measured preoperatively and at postoperative days (POD) 1, 2, 3 and 5. Further, peak serum levels of CRP and lipase during the first 72 h were evaluated. Receiver operating characteristics (ROC) curves were performed to assess their predictive value for ePGD and eRGD. Cut-off levels were calculated with the Youden index. Significant diagnostic biochemical cut-offs as well as other prognostic clinical factors were tested in a multivariate logistic regression model. Results: Of the 105 patients included, 43 patients (41%) and 28 patients (27%) developed ePGD and eRGD following SPKT, respectively. The mean WBC, PCT, NLR, PLR, CRP and lipase levels were significantly higher on most PODs in the ePGD group compared to the non-ePGD group. ROC analysis indicated that peak lipase (AUC: 0.82) and peak CRP levels (AUC: 0.89) were highly predictive for ePGD after SPKT. The combination of both achieved the highest AUC (0.92; p < 0.01) in predicting ePGD. Concerning eRGD, predictive accuracy of all analyzed serological markers was moderate (all AUC < 0.8). Additionally, multivariable analysis identified previous dialysis/no preemptive transplantation (OR 2.4 (95% CI: 1.41−4.01), p = 0.021), donor age (OR 1.07 (95% CI: 1.03−1.14), p < 0.010), donor body mass index (OR 1.32 (95% CI: 1.01−1.072), p = 0.04), donors cerebrovascular cause of death (OR 7.8 (95% CI: 2.21−26.9), p < 0.010), donor length of ICU stay (OR 1.27 (95% CI: 1.08−1.49), p < 0.010), as well as CIT pancreas (OR 1.07 (95% CI: 1.03−1.14), p < 0.010) as clinical relevant prognostic predictors for ePGD. Further, a peak of lipase (OR 1.04 (95% CI: 1.02−1.07), p < 0.010), peak of CRP levels (OR 1.12 (95% CI: 1.02−1.23), p < 0.010), pancreatic serum lipase concentration on POD 2 > 150 IU/L (OR 2.9 (95% CI: 1.2−7.13), p = 0.021) and CRP levels of ≥ 180 ng/mL on POD 2 (OR 3.6 (95% CI: 1.54−8.34), p < 0.01) and CRP levels > 150 ng/mL on POD 3 (OR 4.5 (95% CI: 1.7−11.4), p < 0.01) were revealed as independent biochemical predictive variables for ePGD after transplantation. Conclusions: In the current study, the combination of peak lipase and CRP levels were highly effective in predicting early pancreatic graft dysfunction development following SPKT. In contrast, for early renal graft dysfunction the predictive value of this parameter was less sensitive. Intensified monitoring of these parameters may be helpful for identifying patients at a higher risk of pancreatic ischemia reperfusion injury and various IRI- associated postoperative complications leading to ePGD and thus deteriorated outcome.
尽管在同期胰肾联合移植(SPKT)的围手术期管理方面取得了最新进展和改进,但早期胰腺移植功能障碍(ePGD)仍然是一个关键问题,严重损害早期和长期移植功能及预后。因此,我们评估了一组经典血清标志物在预测接受SPKT患者早期移植功能障碍方面的价值。方法:回顾性分析了1998年至2018年在我们中心接受SPKT的105例患者的前瞻性收集数据库中的医学数据。主要研究结果是检测早期胰腺移植功能障碍(ePGD)的发生情况,次要研究结果是早期肾移植功能障碍(eRGD)以及与移植功能相关的所有其他结果参数。在此背景下,ePGD被定义为胰腺移植相关并发症,包括移植性胰腺炎、胰腺脓肿/腹膜炎、移植功能延迟、移植血栓形成、出血、排斥反应以及因移植相关并发症在3个月内连续需要再次剖腹手术。关于分析ePGD,术前以及术后第1、2、3和5天测量血清白细胞计数(WBC)、C反应蛋白(CRP)、降钙素原(PCT)、胰腺脂肪酶以及中性粒细胞与淋巴细胞比率(NLR)和血小板与淋巴细胞比率(PLR)。此外,评估了前72小时内CRP和脂肪酶的血清峰值水平。绘制受试者工作特征(ROC)曲线以评估它们对ePGD和eRGD的预测价值。使用约登指数计算临界值。在多变量逻辑回归模型中测试了显著的诊断生化临界值以及其他预后临床因素。结果:在纳入的105例患者中,分别有43例患者(41%)和28例患者(27%)在SPKT后发生了ePGD和eRGD。与非ePGD组相比,ePGD组在大多数术后天数的平均WBC、PCT、NLR、PLR、CRP和脂肪酶水平显著更高。ROC分析表明,脂肪酶峰值(AUC:0.82)和CRP峰值水平(AUC:0.89)对SPKT后的ePGD具有高度预测性。两者结合在预测ePGD方面达到了最高的AUC(0.92;p < 0.01)。关于eRGD,所有分析的血清学标志物的预测准确性中等(所有AUC < 0.8)。此外,多变量分析确定既往透析/未进行抢先移植(OR 2.4(95% CI:1.41 - 4.01),p = 0.021)、供体年龄(OR 1.07(95% CI:1.03 - 1.14),p < 0.010)、供体体重指数(OR 1.32(95% CI:1.01 - 1.072),p = 0.04)、供体脑血管死亡原因(OR 7.8(95% CI:2.21 - 26.9),p < 0.010)、供体ICU住院时间(OR 1.27(95% CI:1.08 - 1.49),p < 0.010)以及胰腺冷缺血时间(OR 1.07(95% CI:1.03 - 1.14),p < 0.010)作为ePGD的临床相关预后预测指标。此外,脂肪酶峰值(OR 1.04(95% CI:1.02 - 1.07),p < 0.010)、CRP峰值水平(OR 1.12(95% CI:1.02 - 1.23),p < 0.010)、术后第2天胰腺血清脂肪酶浓度> 150 IU/L(OR 2.9(95% CI:1.2 - 7.13),p = 0.021)以及术后第2天CRP水平≥ 180 ng/mL(OR 3.6(95% CI:1.54 - 8.34),p < 0.01)和术后第3天CRP水平> 150 ng/mL(OR 4.5(95% CI:1.7 - 11.4),p < 0.01)被揭示为移植后ePGD的独立生化预测变量。结论:在本研究中,脂肪酶峰值和CRP水平的组合在预测SPKT后早期胰腺移植功能障碍的发生方面非常有效。相比之下,对于早期肾移植功能障碍,该参数的预测价值不太敏感。加强对这些参数的监测可能有助于识别胰腺缺血再灌注损伤及各种与IRI相关的术后并发症导致ePGD从而预后恶化风险较高的患者。