Department of Neonatology, Shandong Provincial Hospital, Cheeloo College of Medicine, Shandong University, Jinan, 250021, Shandong, China.
Department of Neonatology, Shandong Provincial Hospital Affiliated to Shandong First Medical University, Jinan, 250021, China.
BMC Pediatr. 2022 May 14;22(1):281. doi: 10.1186/s12887-022-03310-5.
Admission hypothermia (AH, < 36.5℃) remains a major challenge for global neonatal survival, especially in developing countries. Baseline research shows nearly 89.3% of very low birth weight (VLBW, < 1500 g) infants suffer from AH in China. Therefore, a prospective multicentric quality improvement (QI) initiative to reduce regional AH and improve outcomes among VLBW neonates was implemented.
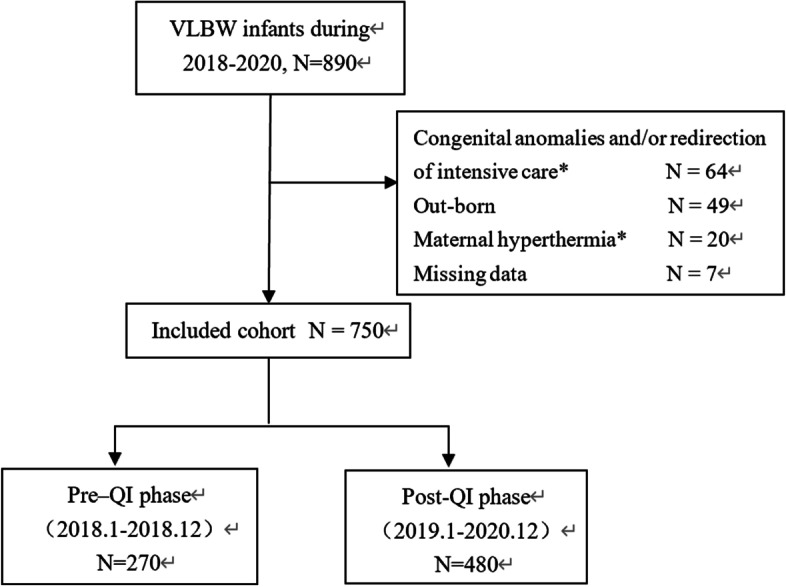
The study used a sequential Plan-Do-Study-Act (PDSA) approach. Clinical data were collected prospectively from 5 NICUs within the Sino-Northern Neonatal Network (SNN) in China. The hypothermia prevention bundle came into practice on January 1, 2019. The clinical characteristics and outcomes data in the pre-QI phase (January 1, 2018- December 31, 2018) were compared with that from the post-QI phase (January 1, 2019-December 31, 2020). Clinical characteristics and outcomes data were analyzed.
A total of 750 in-born VLBW infants were enrolled in the study, 270 in the pre-QI period and 480 in the post- QI period, respectively. There were no significant differences in clinical characteristics of infants between these two phases. Compared with pre-QI period, the incidence of AH was decreased significantly after the QI initiative implementation in the post-QI period (95.9% vs. 71.3%, P < 0.01). Incidence of admission moderate-to-severe hypothermia (AMSH, < 36℃) also decreased significantly, manifesting a reduction to 38.5% in the post-QI (68.5% vs 30%, P < 0.01). Average admission temperature improved from after QI (35.5 [Formula: see text] 0.7℃ vs. 36.0 [Formula: see text] 0.6℃, P < 0.01). There was no increase in proportion the number of infants with a temperature of > 37.5 °C or thermal burns between the two groups. The risk ratio of mortality in infants during the post-QI period was significantly lower in the post-QI period as compared to the pre-QI period [adjusted risk ratio (aRR): 0.26, 95% confidence interval (CI): 0.13-0.50]. The risk ratio of late-onset neonatal sepsis (LOS) also significantly lowered in the post-QI period (aRR: 0.66, 95% CI: 0.50-0.87).
Implementation of multicentric thermoregulatory QI resulted in a significant reduction in AH and AMSH in VLBW neonates with associated reduction in mortality. We gained a lot from the QI, and successfully aroused the attention of perinatal medical staff to neonatal AH. This provided a premise for continuous quality improvement of AH in the future, and might provide a reference for implementation of similar interventions in developing countries.
Trial registration number: ChiCTR1900020861 . Date of registration: 21 January 2019(21/01/2019). Prospectively registered.
入院低体温(AH,<36.5℃)仍然是全球新生儿存活的主要挑战,尤其是在发展中国家。基线研究表明,中国近 89.3%的极低出生体重(VLBW,<1500 g)婴儿存在 AH。因此,实施了一项前瞻性多中心质量改进(QI)计划,以降低区域性 AH 并改善 VLBW 新生儿的结局。
本研究采用了计划-实施-研究-行动(PDSA)的顺序方法。临床数据前瞻性地从中国北方新生儿网络(SNN)内的 5 个 NICU 收集。低体温预防包于 2019 年 1 月 1 日开始实施。比较了 QI 前阶段(2018 年 1 月 1 日至 12 月 31 日)和 QI 后阶段(2019 年 1 月 1 日至 12 月 31 日)的临床特征和结局数据。分析了临床特征和结局数据。
共纳入 750 例足月 VLBW 婴儿,QI 前阶段 270 例,QI 后阶段 480 例。这两个阶段婴儿的临床特征无显著差异。与 QI 前阶段相比,QI 后阶段的 AH 发生率显著降低(95.9% vs. 71.3%,P<0.01)。中度至重度入院低体温(AMSH,<36℃)的发生率也显著降低,QI 后为 38.5%(68.5% vs 30%,P<0.01)。入院平均体温在 QI 后有所改善(35.5[公式:见正文]0.7℃ vs. 36.0[公式:见正文]0.6℃,P<0.01)。两组间体温>37.5℃或热烧伤的婴儿比例无增加。QI 后阶段婴儿死亡率的风险比明显低于 QI 前阶段[调整风险比(aRR):0.26,95%置信区间(CI):0.13-0.50]。QI 后阶段新生儿晚发性败血症(LOS)的风险比也明显降低(aRR:0.66,95%CI:0.50-0.87)。
多中心体温调节 QI 的实施显著降低了 VLBW 新生儿的 AH 和 AMSH,死亡率也随之降低。我们从 QI 中获益良多,成功引起了围产期医务人员对新生儿 AH 的关注。这为未来 AH 的持续质量改进提供了前提,并可能为发展中国家实施类似干预措施提供参考。
临床试验注册号:ChiCTR1900020861。注册日期:2019 年 1 月 21 日(21/01/2019)。前瞻性注册。