Muir Matthew, Rhines Laurence, Demonte Franco, Tatsui Claudio, Raza Shaan M
Department of Neurosurgery, The University of Texas MD Anderson Cancer Center, Houston, TX, USA.
Neurospine. 2022 Jun;19(2):434-440. doi: 10.14245/ns.2244034.017. Epub 2022 May 15.
Spinal reconstruction after resection of invasive craniocervical junction malignancies is fraught with technical and management considerations as well as a paucity of data in the existing literature. In this study, we describe our experience with craniocervical junction malignancies, especially the influence of radiation on the need for revision spinal instrumentation.
We performed a retrospective chart review of all patients who underwent occipitocervical fixation between 2011 and 2019 at The University of Texas MD Anderson Cancer Center.
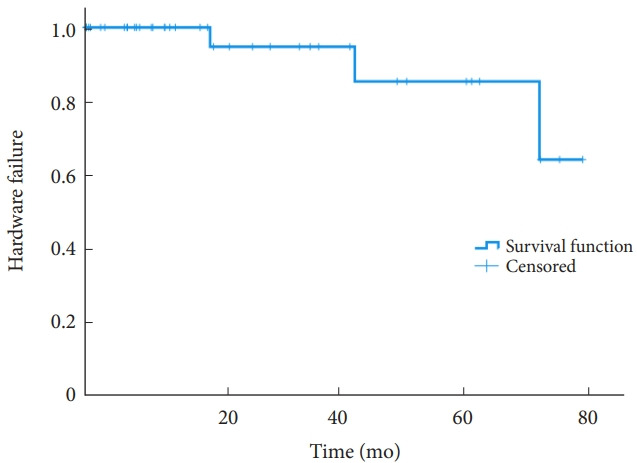
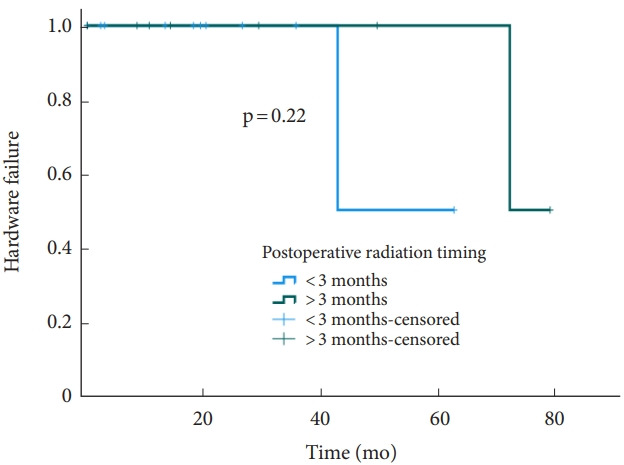
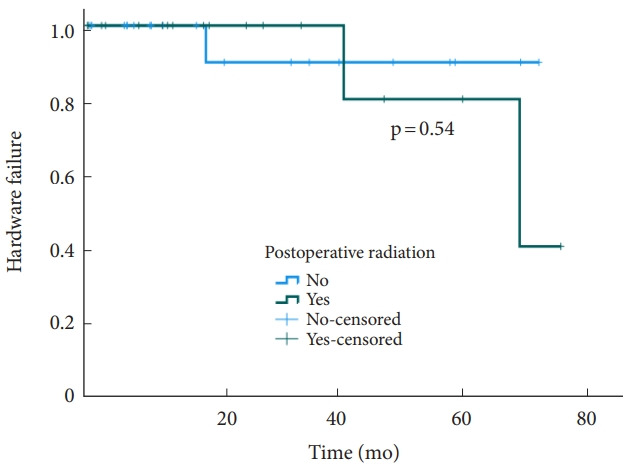
Twenty-five patients had primary malignancies and 12 (30%) had metastatic tumors. Thirteen (33%) underwent a staged resection in multiple operations during their hospital stay. Tumor resection was performed in 19 patients (48%), while only stabilization was performed in 21 patients (52%). Nine patients (23%) underwent expanded endoscopic transclival approaches for tumor resection, 10 patients (25%) an extreme lateral approach, and 2 patients (5%) an anterior open approach. Eleven patients underwent early postoperative radiation therapy (within 3 months) and 8 underwent delayed radiation therapy (between 3 months and 1 year in 7 patients). The revision rate was 8%, with a median time to revision surgery of 42 months. The administration and timing of adjuvant radiation therapy relative to surgery had no significant effect on the need for instrumentation revision on log-rank and Cox regression analyses (p < 0.05).
Revision surgery was needed infrequently in our patients. Postoperative radiation therapy was not associated with hardware failure, indicating that the timing of radiation therapy should be dictated by the diagnosis and can be initiated postoperatively without delay.
侵袭性颅颈交界区恶性肿瘤切除术后的脊柱重建充满了技术和管理方面的考量,且现有文献中的数据匮乏。在本研究中,我们描述了我们在颅颈交界区恶性肿瘤方面的经验,尤其是放疗对翻修脊柱内固定需求的影响。
我们对2011年至2019年在德克萨斯大学MD安德森癌症中心接受枕颈固定的所有患者进行了回顾性病历审查。
25例患者患有原发性恶性肿瘤,12例(30%)患有转移性肿瘤。13例(33%)在住院期间分多次手术进行了分期切除。19例患者(48%)进行了肿瘤切除,而仅21例患者(52%)进行了稳定手术。9例患者(23%)采用扩大的内镜经斜坡入路进行肿瘤切除,10例患者(25%)采用极外侧入路,2例患者(5%)采用前路开放入路。11例患者在术后早期(3个月内)接受放疗治疗,8例患者接受延迟放疗(7例患者在3个月至1年之间)。翻修率为8%,翻修手术的中位时间为42个月。在对数秩检验和Cox回归分析中,辅助放疗相对于手术的给药和时间安排对器械翻修需求无显著影响(p<0.05)。
我们的患者很少需要进行翻修手术。术后放疗与内固定失败无关,这表明放疗时间应由诊断决定,并且可以在术后立即开始。