The Department of Cardiovascular Medicine, The University of Tokyo, 7-3-1, Hongo, Bunkyo-ku, Tokyo, 113-8655, Japan.
Department of Rehabilitation Sciences, Kitasato University Graduate School of Medical Sciences, Sagamihara, Japan.
Cardiovasc Diabetol. 2022 May 18;21(1):67. doi: 10.1186/s12933-022-01508-6.
There have been scarce data comparing cardiovascular outcomes between individual sodium-glucose cotransporter-2 (SGLT2) inhibitors. We aimed to compare the subsequent cardiovascular risk between individual SGLT2 inhibitors.
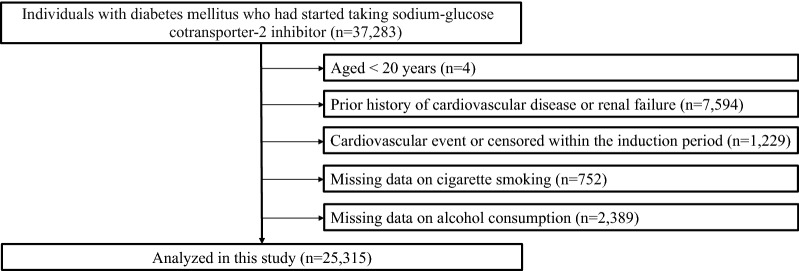
We analyzed 25,315 patients with diabetes mellitus (DM) newly taking SGLT2 inhibitors (empagliflozin: 5302, dapagliflozin: 4681, canagliflozin: 4411, other SGLT2 inhibitors: 10,921). We compared the risks of developing heart failure (HF), myocardial infarction (MI), angina pectoris (AP), stroke, and atrial fibrillation (AF) between individual SGLT2 inhibitors.
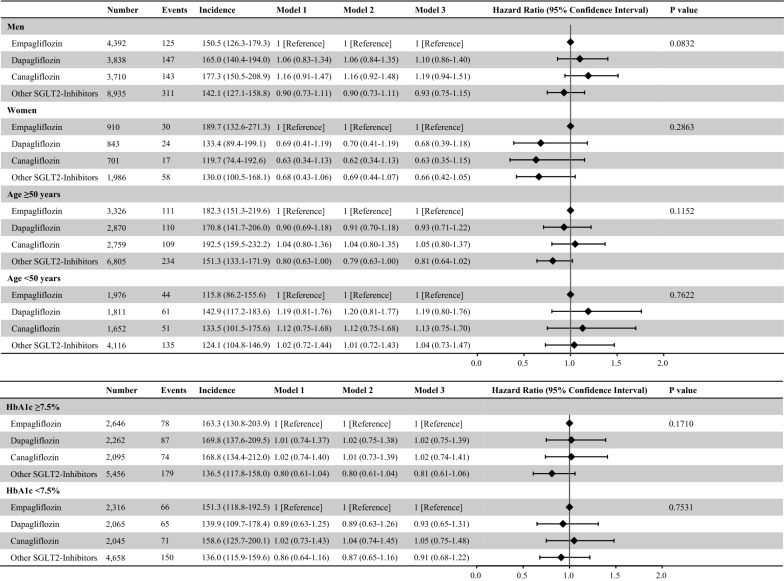
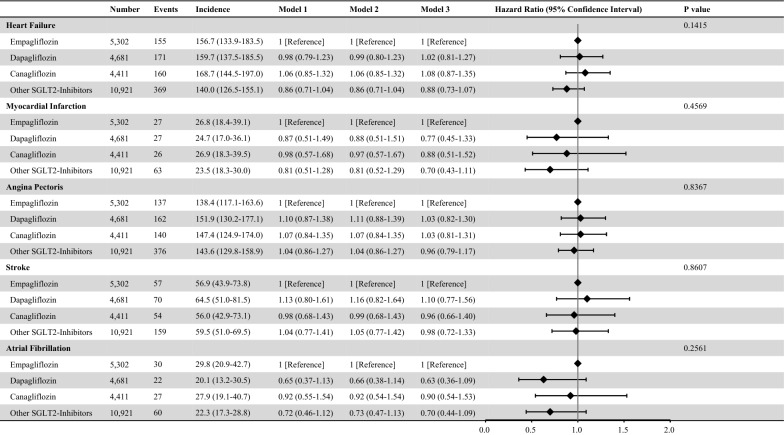
Median age was 52 years, and 82.5% were men. The median fasting plasma glucose and HbA1c levels were 149 (Q1-Q3:127-182) mg/dL and 7.5 (Q1-Q3:6.9-8.6) %. During a mean follow-up of 814 ± 591 days, 855 HF, 143 MI, 815 AP, 340 stroke, and 139 AF events were recorded. Compared with empagliflozin, the risk of developing HF, MI, AP, stroke, and AF was not significantly different in dapagliflozin, canagliflozin, and other SGLT inhibitors. For developing HF, compared with empagliflozin, hazard ratios of dapagliflozin, canagliflozin, and other SGLT2 inhibitors were 1.02 (95% confidence interval [CI] 0.81-1.27), 1.08 (95% CI 0.87-1.35), and 0.88 (95% CI 0.73-1.07), respectively. Wald tests showed that there was no significant difference in the risk of developing HF, MI, AP, stroke, and AF among individual SGLT2 inhibitors. We confirmed the robustness of these results through a multitude of sensitivity analyses.
The risks for subsequent development of HF, MI, AP, stroke, and AF were comparable between individual SGLT2 inhibitors. This is the first study comparing the wide-range cardiovascular outcomes of patients with DM treated with individual SGLT2 inhibitors using large-scale real-world data.
比较不同钠-葡萄糖共转运蛋白 2(SGLT2)抑制剂对心血管结局影响的数据较为匮乏。本研究旨在比较不同 SGLT2 抑制剂对心血管的后续风险。
本研究纳入 25315 例新服用 SGLT2 抑制剂的糖尿病(DM)患者(恩格列净:5302 例,达格列净:4681 例,卡格列净:4411 例,其他 SGLT2 抑制剂:10921 例)。我们比较了不同 SGLT2 抑制剂发生心力衰竭(HF)、心肌梗死(MI)、心绞痛(AP)、卒中和心房颤动(AF)的风险。
中位年龄为 52 岁,82.5%为男性。中位空腹血糖和糖化血红蛋白(HbA1c)水平分别为 149(Q1-Q3:127-182)mg/dL 和 7.5(Q1-Q3:6.9-8.6)%。平均随访 814±591 天后,共记录到 855 例 HF、143 例 MI、815 例 AP、340 例卒中和 139 例 AF 事件。与恩格列净相比,达格列净、卡格列净和其他 SGLT 抑制剂发生 HF、MI、AP、卒中和 AF 的风险无显著差异。对于 HF 的发生,与恩格列净相比,达格列净、卡格列净和其他 SGLT2 抑制剂的风险比(HR)分别为 1.02(95%置信区间[CI]:0.81-1.27)、1.08(95%CI:0.87-1.35)和 0.88(95%CI:0.73-1.07)。Wald 检验显示,不同 SGLT2 抑制剂之间 HF、MI、AP、卒中和 AF 的发生风险无显著差异。通过大量敏感性分析证实了这些结果的稳健性。
在 DM 患者中,不同 SGLT2 抑制剂对 HF、MI、AP、卒中和 AF 发生的后续风险相似。这是第一项使用大规模真实世界数据比较接受不同 SGLT2 抑制剂治疗的 DM 患者广泛心血管结局的研究。