Department of Urology, The Jikei University School of Medicine, 3-19-18, Nishi-shimbashi, Minato-ku, Tokyo, 105-8471, Japan.
Department of Urology, Comprehensive Cancer Center, Medical University of Vienna, Vienna, Austria.
World J Urol. 2023 Aug;41(8):2051-2062. doi: 10.1007/s00345-022-04030-2. Epub 2022 May 21.
The aim of this study was to investigate the oncologic efficacy of combining docetaxel with androgen deprivation therapy (ADT) versus nonsteroidal antiandrogen (NSAA) with ADT in patients with high-volume metastatic hormone-sensitive prostate cancer (mHSPC) with focus on the effect of sequential therapy in a real-world clinical practice setting.
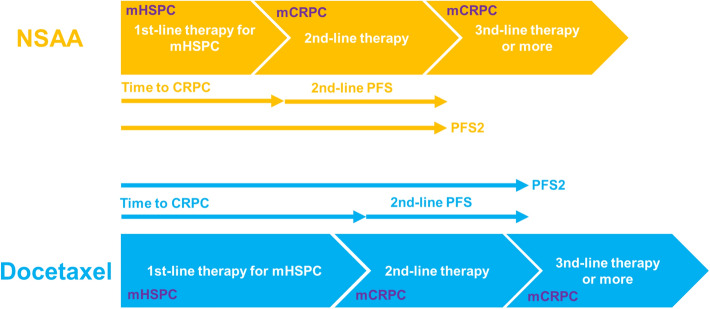
The records of 382 patients who harbored high-volume mHSPC, based on the CHAARTED criteria, and had received ADT with either docetaxel (n = 92) or NSAA (bicalutamide) (n = 290) were retrospectively analyzed. The cohorts were matched by one-to-one propensity scores based on patient demographics. Overall survival (OS), cancer-specific survival (CSS), progression-free survival (PFS), including time to castration-resistant prostate cancer (CRPC), and time to second-line progression (PFS2) were compared. 2nd-line PFS defined as the time from CRPC diagnosis to progression after second-line therapy was also compared.
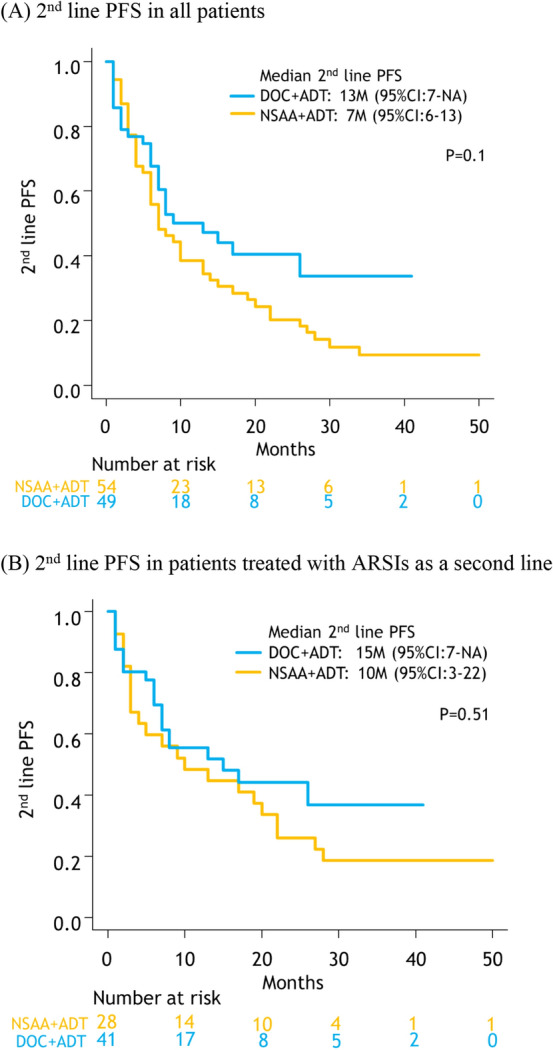
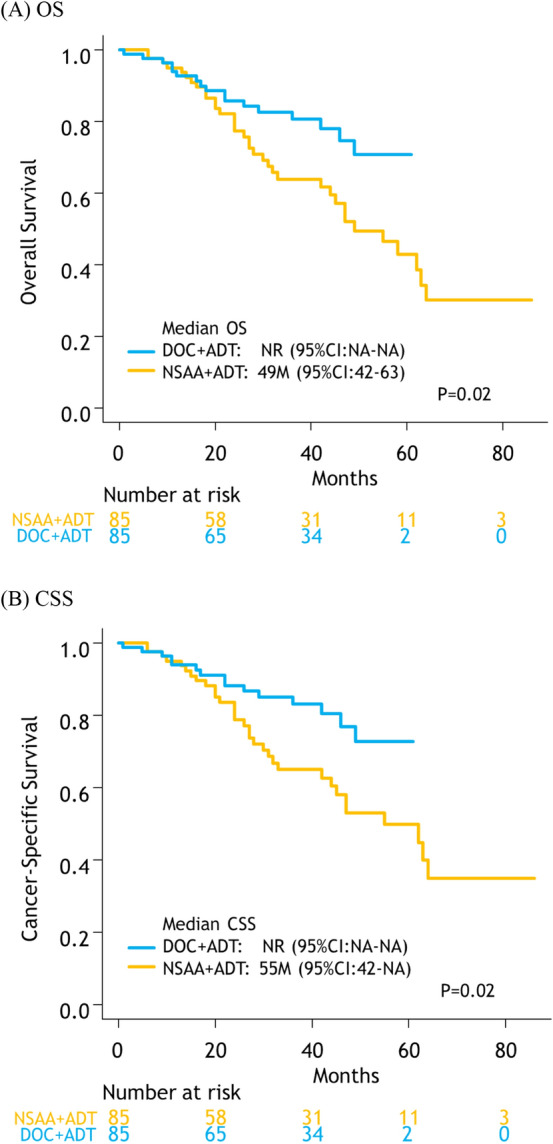
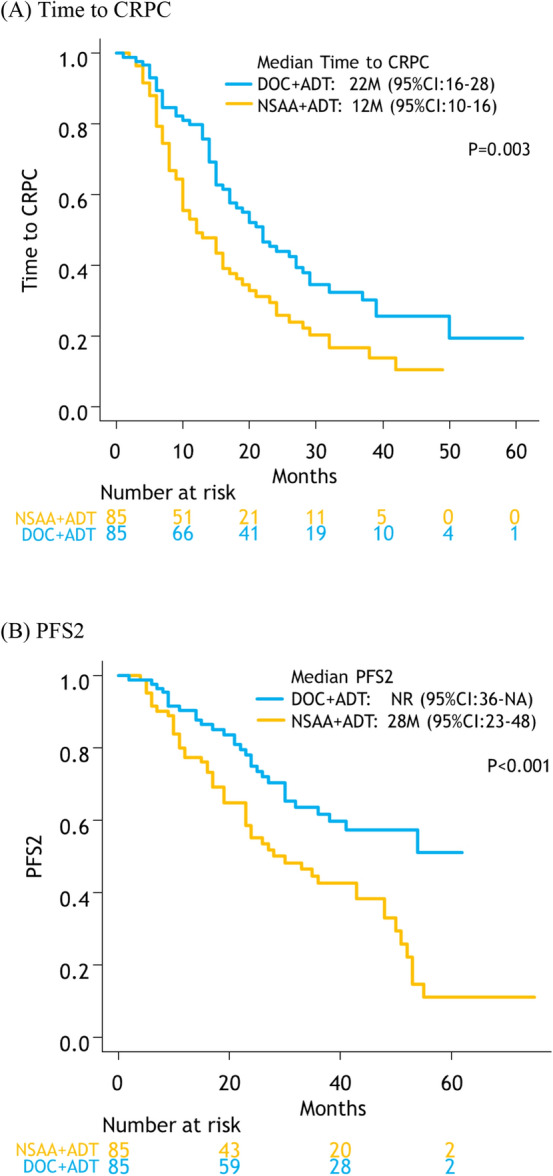
After matching, a total of 170 patients were retained: 85 patients treated with docetaxel + ADT and 85 patients treated with NSAA + ADT. The median OS and CSS for docetaxel + ADT versus NSAA + ADT were not reached (NR) vs. 49 months (p = 0.02) and NR vs. 55 months (p = 0.02), respectively. Median time to CRPC and PFS2 in patients treated with docetaxel + ADT was significantly longer compared to those treated with NSAA (22 vs. 12 months; p = 0.003 and, NR vs. 28 months; p < 0.001, respectively). There was no significant difference in 2nd-line PFS between the two groups.
Our analysis suggested that ADT with docetaxel significantly prolonged OS and CSS owing to a better time to CRPC and PFS2 in comparison to NSAA + ADT in high-volume mHSPC.
本研究旨在探讨在符合 CHAARTED 标准的高瘤负荷转移性去势敏感性前列腺癌(mHSPC)患者中,与非甾体类抗雄激素(NSAA)联合去势治疗(ADT)相比,多西他赛联合 ADT 的肿瘤疗效,重点关注真实临床实践环境下序贯治疗的效果。
回顾性分析了 382 例符合 CHAARTED 标准的高瘤负荷 mHSPC 患者的记录,他们接受了 ADT 联合多西他赛(n=92)或 NSAA(比卡鲁胺)(n=290)。根据患者的人口统计学特征,通过一对一倾向评分匹配队列。比较总生存期(OS)、癌症特异性生存期(CSS)、无进展生存期(PFS),包括去势抵抗性前列腺癌(CRPC)时间和二线进展时间(PFS2)。还比较了从 CRPC 诊断到二线治疗后进展的二线 PFS 时间。
匹配后,共保留了 170 例患者:85 例接受多西他赛+ADT 治疗,85 例接受 NSAA+ADT 治疗。多西他赛+ADT 组与 NSAA+ADT 组的中位 OS 和 CSS 均未达到(NR)vs.49 个月(p=0.02)和 NR vs.55 个月(p=0.02)。多西他赛+ADT 组患者的 CRPC 时间和 PFS2 时间明显长于 NSAA 组(22 个月 vs.12 个月;p=0.003 和 NR vs.28 个月;p<0.001)。两组间二线 PFS 无显著差异。
我们的分析表明,与 NSAA+ADT 相比,多西他赛联合 ADT 可显著延长 OS 和 CSS,因为与 NSAA+ADT 相比,多西他赛联合 ADT 可使 CRPC 时间和 PFS2 时间更好。