Department of Oral and Maxillofacial Surgery, Sun Yat-Sen Memorial Hospital, Sun Yat-Sen University, 107th Yanjiang Xi Road, Guangzhou, 510120, Guangdong, China.
Department of Stomatology, Longgang District Central Hospital, Shenzhen, 518116, Guangdong, China.
BMC Oral Health. 2022 May 28;22(1):213. doi: 10.1186/s12903-022-02244-9.
To assess the contributing risk factors for the progression of, and the postoperative poor prognosis associated with, osteoradionecrosis of jaw (ORNJ) following non-nasopharyngeal cancer treatment in head and neck.
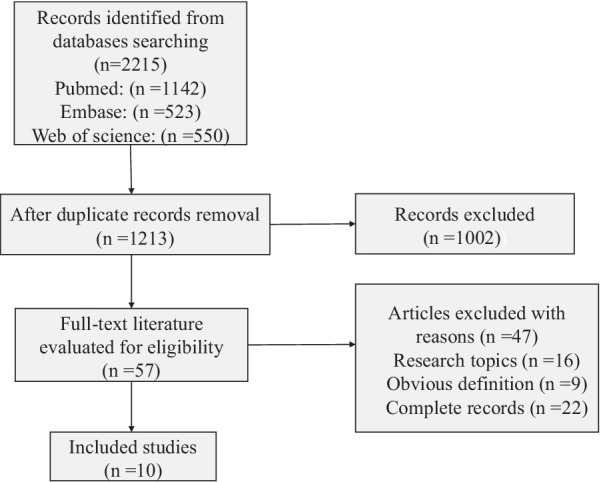
A retrospective study of 124 non-nasopharyngeal carcinoma patients in head and neck treated at one institution between 2001 and 2020 was conducted. A cumulative meta-analysis was conducted according to PRISMA protocol and the electronic search was performed on the following search engines: PubMed, Embase, and Web of Science. After assessing surgery with jaw lesions as a risk factor for the occurrence of ORNJ, 124 cases were categorized into two groups according to the "BS" classification, after which jaw lesions, chemotherapy, flap reconstruction and onset time of ORNJ were analyzed through the chi-square test and t-test to demonstrate the potential association between them and the progression of ORNJ. Postoperative outcomes of wound healing, occlusal disorders, and nerve injury were statistically analyzed.
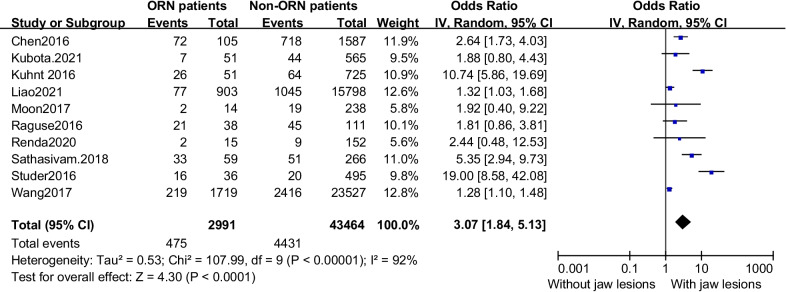
With the statistically significant results of the meta-analysis (odds ratio = 3.07, 95% CI: 1.84-5.13, p < 0.0001), the chi-square test and t-test were used to validate our hypotheses and identified that surgery with jaw lesions could aggravate the progression and accelerate the appearance of ORNJ. Patients who underwent chemotherapy tended to suffer from severe-to-advanced osteonecrosis but did not shorten the onset time of ORNJ. Flap reconstruction presented obvious advantages in wound healing (p < 0.001) and disordered occlusion (p < 0.005). The mean onset time of ORNJ in non-nasopharyngeal cancer patients (4.5 years) was less than that in patients with nasopharyngeal cancer (NPC) (6.8 years).
Iatrogenic jaw lesions are evaluated as a significant risk factor in the occurrence and progression of ORNJ in non-nasopharyngeal carcinoma patients who tend to have more severe and earlier osteonecrosis after radiotherapy than NPC patients. Flap reconstruction is a better choice for protecting the remaining bone tissue and reducing postoperative complications of ORNJ.
评估头颈部非鼻咽癌治疗后颌骨放射性骨坏死(ORNJ)进展的相关危险因素,以及与ORNJ 相关的术后不良预后。
对 2001 年至 2020 年在一家机构治疗的 124 例头颈部非鼻咽癌患者进行回顾性研究。根据 PRISMA 方案进行累积荟萃分析,并在以下搜索引擎上进行电子检索:PubMed、Embase 和 Web of Science。在评估颌骨病变作为 ORNJ 发生的危险因素的手术后,根据“BS”分类将 124 例病例分为两组,然后通过卡方检验和 t 检验分析颌骨病变、化疗、皮瓣重建和 ORNJ 的发病时间,以证明它们与 ORNJ 进展之间的潜在关联。对伤口愈合、咬合紊乱和神经损伤的术后结果进行统计学分析。
荟萃分析的统计学结果具有显著性(比值比 = 3.07,95%置信区间:1.84-5.13,p < 0.0001),卡方检验和 t 检验用于验证我们的假设,并确定颌骨病变的手术会加重进展并加速 ORNJ 的出现。接受化疗的患者往往患有严重到晚期的骨坏死,但不会缩短 ORNJ 的发病时间。皮瓣重建在伤口愈合(p < 0.001)和咬合紊乱(p < 0.005)方面具有明显优势。非鼻咽癌患者的 ORNJ 平均发病时间(4.5 年)短于鼻咽癌(NPC)患者(6.8 年)。
医源性颌骨病变被评估为非鼻咽癌患者发生和进展 ORNJ 的显著危险因素,这些患者在接受放疗后比 NPC 患者更容易发生更严重和更早的骨坏死。皮瓣重建是保护剩余骨组织和减少 ORNJ 术后并发症的更好选择。