Volovici Victor, Pisică Dana, Gravesteijn Benjamin Y, Dirven Clemens M F, Steyerberg Ewout W, Ercole Ari, Stocchetti Nino, Nelson David, Menon David K, Citerio Giuseppe, van der Jagt Mathieu, Maas Andrew I R, Haitsma Iain K, Lingsma Hester F
Department of Neurosurgery, Erasmus MC, Rotterdam, The Netherlands.
Department of Public Health, Center for Medical Decision Making, Erasmus MC University Medical Center, Erasmus MC Stroke Center, Doctor Molewaterplein 40, 3015 GD, Rotterdam, The Netherlands.
Acta Neurochir (Wien). 2022 Jul;164(7):1693-1705. doi: 10.1007/s00701-022-05257-z. Epub 2022 Jun 1.
To compare outcomes between patients with primary external ventricular device (EVD)-driven treatment of intracranial hypertension and those with primary intraparenchymal monitor (IP)-driven treatment.
The CENTER-TBI study is a prospective, multicenter, longitudinal observational cohort study that enrolled patients of all TBI severities from 62 participating centers (mainly level I trauma centers) across Europe between 2015 and 2017. Functional outcome was assessed at 6 months and a year. We used multivariable adjusted instrumental variable (IV) analysis with "center" as instrument and logistic regression with covariate adjustment to determine the effect estimate of EVD on 6-month functional outcome.
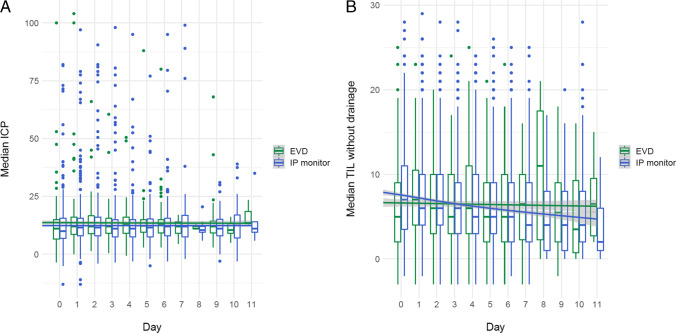
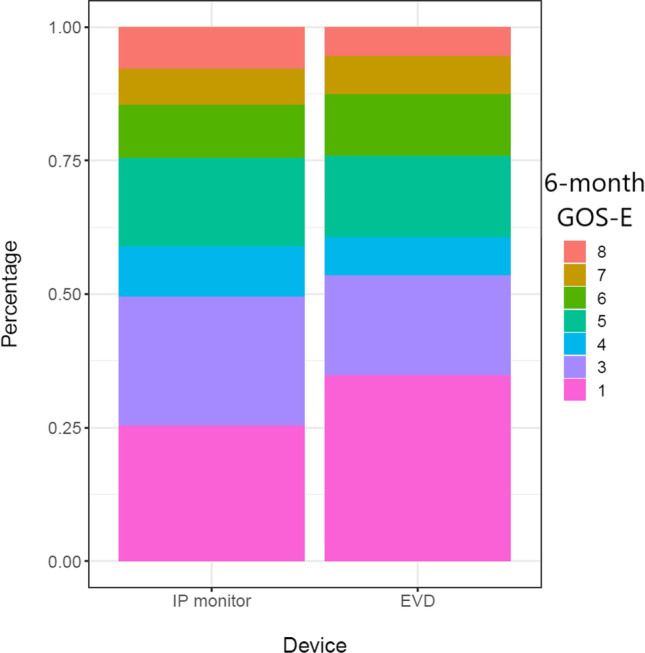
A total of 878 patients of all TBI severities with an indication for intracranial pressure (ICP) monitoring were included in the present study, of whom 739 (84%) patients had an IP monitor and 139 (16%) an EVD. Patients included were predominantly male (74% in the IP monitor and 76% in the EVD group), with a median age of 46 years in the IP group and 48 in the EVD group. Six-month GOS-E was similar between IP and EVD patients (adjusted odds ratio (aOR) and 95% confidence interval [CI] OR 0.74 and 95% CI [0.36-1.52], adjusted IV analysis). The length of intensive care unit stay was greater in the EVD group than in the IP group (adjusted rate ratio [95% CI] 1.70 [1.34-2.12], IV analysis). One hundred eighty-seven of the 739 patients in the IP group (25%) required an EVD due to refractory ICPs.
We found no major differences in outcomes of patients with TBI when comparing EVD-guided and IP monitor-guided ICP management. In our cohort, a quarter of patients that initially received an IP monitor required an EVD later for ICP control. The prevalence of complications was higher in the EVD group.
The core study is registered with ClinicalTrials.gov , number NCT02210221, and the Resource Identification Portal (RRID: SCR_015582).
比较原发性采用脑室外引流装置(EVD)治疗颅内高压的患者与原发性采用脑实质内监测器(IP)治疗的患者的治疗结果。
CENTER-TBI研究是一项前瞻性、多中心、纵向观察性队列研究,在2015年至2017年期间纳入了来自欧洲62个参与中心(主要是一级创伤中心)的所有创伤性脑损伤严重程度的患者。在6个月和1年时评估功能结局。我们使用以“中心”为工具的多变量调整工具变量(IV)分析和有协变量调整的逻辑回归来确定EVD对6个月功能结局的效应估计。
本研究共纳入878例有颅内压(ICP)监测指征的所有创伤性脑损伤严重程度的患者,其中739例(84%)患者使用IP监测器,139例(16%)使用EVD。纳入的患者以男性为主(IP监测器组为74%,EVD组为76%),IP组中位年龄为46岁,EVD组为48岁。IP组和EVD组患者6个月的扩展格拉斯哥预后量表(GOS-E)相似(调整优势比(aOR)及95%置信区间[CI],OR为0.74,95%CI为[0.36 - 1.52],调整IV分析)。EVD组重症监护病房住院时间比IP组长(调整率比[95%CI]为1.70[1.34 - 2.12],IV分析)。IP组739例患者中有187例(25%)因难治性ICP需要使用EVD。
比较EVD引导和IP监测引导的ICP管理时,我们发现创伤性脑损伤患者的治疗结果无重大差异。在我们的队列中,最初接受IP监测的患者中有四分之一后来因ICP控制需要使用EVD。EVD组并发症发生率更高。
核心研究已在ClinicalTrials.gov注册,编号为NCT02210221,以及资源识别门户(RRID:SCR_015582)。