Chalidis Byron E, Sachinis Nick P, Hawdon Gabrielle, McMahon Stephen
Malabar Orthopaedic Clinic, 43 The Avenue, Windsor, Melbourne, 3181, Australia.
Arthroplasty. 2022 Jun 6;4(1):26. doi: 10.1186/s42836-022-00127-6.
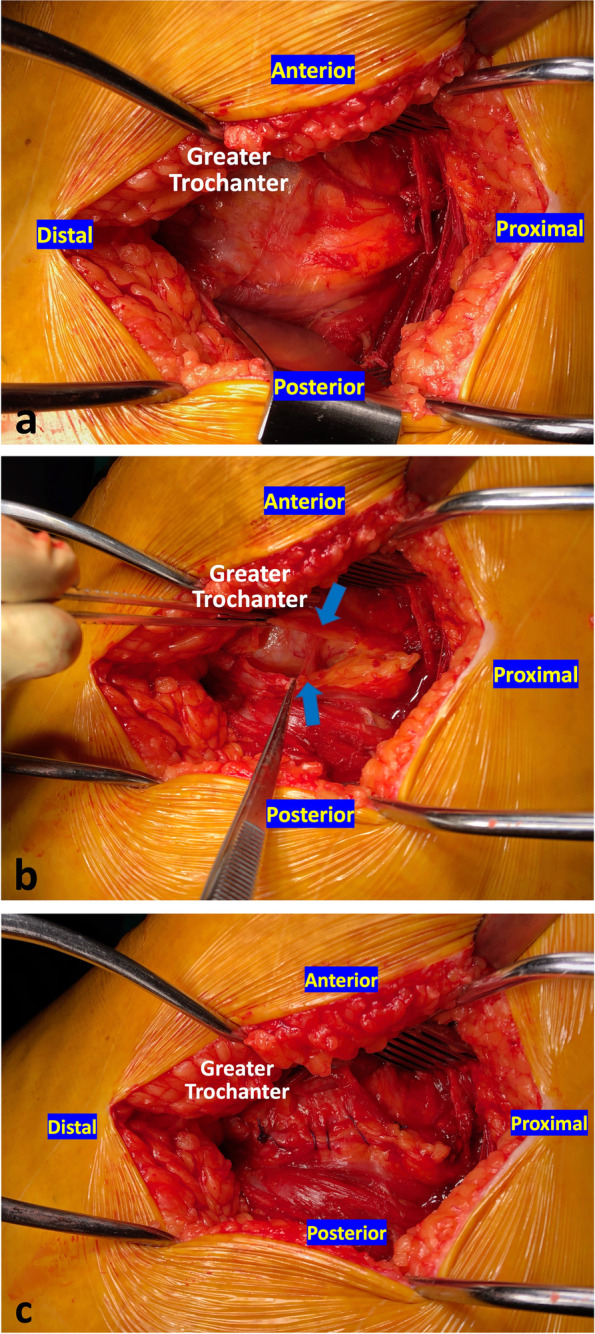
The trochanteric bursa (TB) is an anatomic structure, which is dissected during posterior/lateral hip approaches in Total Hip Arthroplasty (THA). Some surgeons prefer to simply resect the bursa as they believe that it may be responsible for postoperative lateral trochanteric pain (LTP). Others advocate that this tissue acts as a buffer minimizing friction between soft tissue and bone, and therefore its repair may prevent LTP after THA.
The purpose of this prospective randomized controlled trial was to compare the clinical results of either resecting or repairing the TB during posterior approach THA.
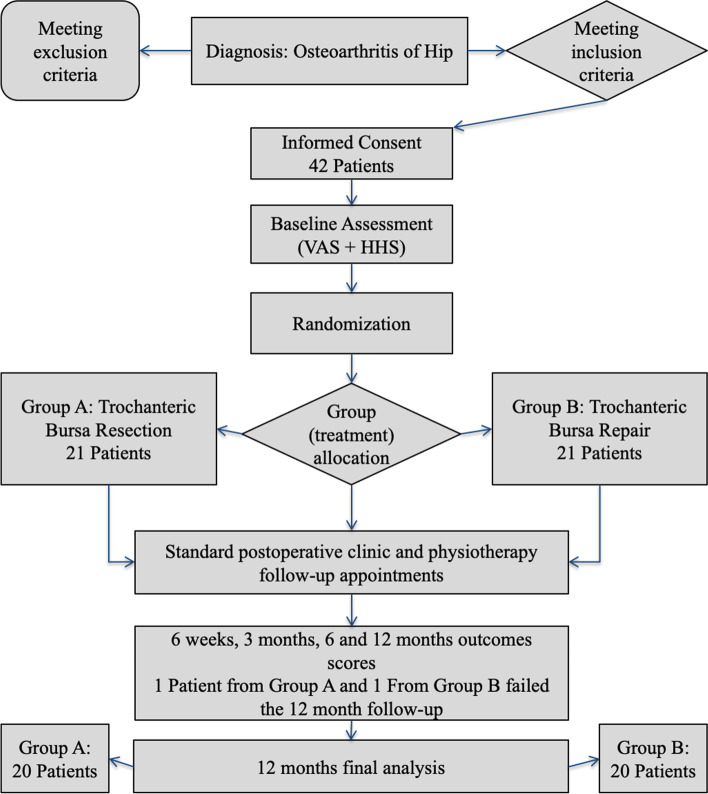
Forty-two patients with primary hip osteoarthritis undergoing THA via a posterior hip approach were randomly assigned to two groups; Group A, or TB resection group and Group B, or TB repair group. All patients in both groups were evaluated postoperatively in terms of hip function, measured by the Harris Hip Score (HHS), at 6 weeks, 3 months, 6 months, and 12 months after surgery, as well as LTP during daily routine activities and lying on the operative side.
Forty patients completed the study. Postoperative difference in terms of leg length and femoral offset was similar among the two groups (P = 0.467 and P = 0.39, respectively). At 6 weeks, patients in Group B had higher HHS (P = 0.052) and experienced less LTP when lying on the operative side (P = 0.046) but not during activities (P = 0.759). Thereafter, all functional parameters measured had comparable values in both groups. Subgroup analysis failed to identify any correlation between high offset stems and LTP.
TB repair in posterior approach THA improves hip functional recovery as well as patients' ability to lie on the operative side during the early postoperative period.
转子囊(TB)是一种解剖结构,在全髋关节置换术(THA)的后外侧入路手术中会被切开。一些外科医生倾向于直接切除该滑囊,因为他们认为它可能是术后外侧转子疼痛(LTP)的原因。另一些人则主张该组织起到缓冲作用,可减少软组织与骨骼之间的摩擦,因此修复它可能预防THA术后的LTP。
这项前瞻性随机对照试验的目的是比较后外侧入路THA术中切除或修复TB的临床效果。
42例因原发性髋关节骨关节炎需行后外侧入路THA的患者被随机分为两组;A组,即TB切除组和B组,即TB修复组。两组所有患者均在术后6周、3个月、6个月和12个月时通过Harris髋关节评分(HHS)评估髋关节功能,以及评估日常活动和患侧卧位时的LTP情况。
40例患者完成了研究。两组术后下肢长度和股骨偏心距的差异相似(分别为P = 0.467和P = 0.39)。在术后6周时,B组患者的HHS更高(P = 0.052),患侧卧位时LTP更少(P = 0.046),但在活动时无差异(P = 0.759)。此后,两组所有测量的功能参数值相当。亚组分析未发现高偏心距假体柄与LTP之间存在任何相关性。
后外侧入路THA术中修复TB可改善髋关节功能恢复,以及患者术后早期患侧卧位的能力。