Senderovich Helen, Vinoraj Danusha, Stever Madeline, Waicus Sarah
Baycrest, 3560 Bathurst Street, Toronto, ON M6A 2E1, Canada.
Department of Psychiatry, Faculty of Medicine, University of Ottawa, Ottawa, ON, Canada.
Ther Adv Infect Dis. 2022 Jun 1;9:20499361221095666. doi: 10.1177/20499361221095666. eCollection 2022 Jan-Dec.
A majority of the fatalities due to COVID-19 have been observed in those over the age of 60. There is no approved and universally accepted treatment for geriatric patients. The aim of this review is to assess the current literature on efficacy of COVID-19 treatments in geriatric populations.
A systematic review search was conducted in PubMed, MedRxiv, and JAMA databases with the keywords COVID-19, geriatric, hydroxychloroquine, dexamethasone, budesonide, remdesivir, favipiravir, ritonavir, molnupiravir, tocilizumab, bamlanivimab, baricitinib, sotrovimab, fluvoxamine, convalescent plasma, prone position, or anticoagulation. Articles published from January 2019 to January 2022 with a population greater than or equal to 60 years of age were included. Interventions examined included hydroxychloroquine, remdesivir, favipiravir, dexamethasone, budesonide, tocilizumab, bamlanivimab, baricitinib, sotrovimab, convalescent plasma, prone position, and anticoagulation therapy. Outcome measures included viral load, viral markers, ventilator-free days, or clinical improvement.
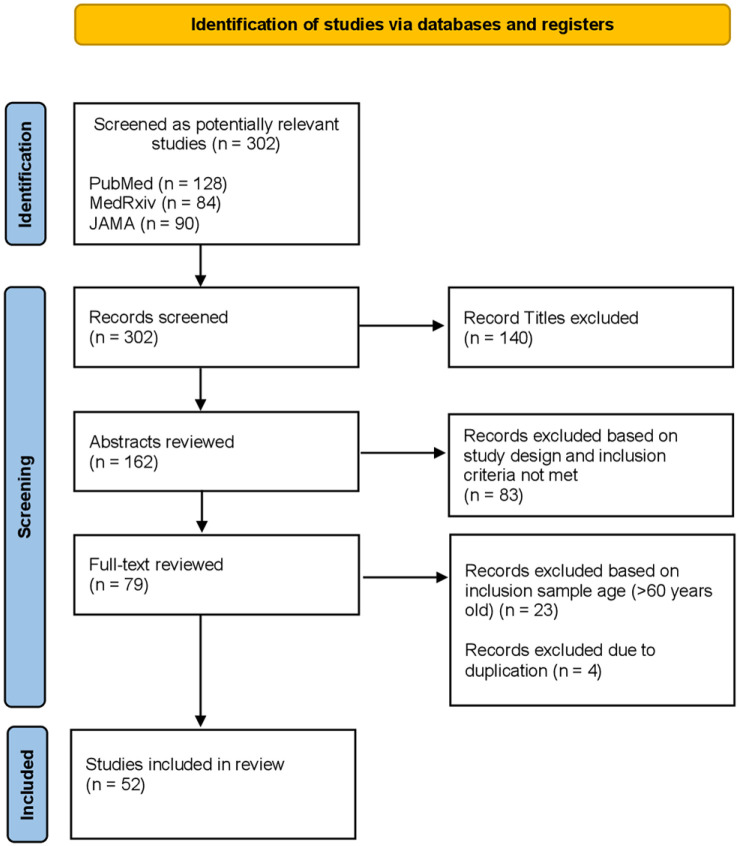
The search revealed 302 articles, 52 met inclusion criteria. Hydroxychloroquine, dexamethasone, and remdesivir revealed greater side effects or inefficiency in geriatric patients with COVID-19. Favipiravir, bamlanivimab, baricitinib, and supportive therapy showed a decrease in viral load and improvement of clinical symptoms. There is conflicting evidence with tocilizumab, convalescent plasma, and anticoagulant therapy in reducing mortality, ventilator-free days, and clinical improvements. In addition, there was limited evidence and lack of data due to ongoing trials for treatments with sotrovimab and budesonide.
No agent is known to be effective for preventing COVID-19 after exposure to the virus. Further research is needed to ensure safety and efficacy of each of the reviewed interventions for older adults.
在因新冠病毒疾病(COVID-19)死亡的病例中,大部分发生在60岁以上的人群。目前尚无针对老年患者的获批且被普遍接受的治疗方法。本综述的目的是评估当前关于COVID-19治疗方法在老年人群中疗效的文献。
在PubMed、MedRxiv和JAMA数据库中进行系统检索,关键词为COVID-19、老年、羟氯喹、地塞米松、布地奈德、瑞德西韦、法匹拉韦、利托那韦、莫努匹拉韦、托珠单抗、巴瑞替尼、索托维单抗、氟伏沙明、康复期血浆、俯卧位或抗凝。纳入2019年1月至2022年1月发表的、研究人群年龄大于或等于60岁的文章。所研究的干预措施包括羟氯喹、瑞德西韦、法匹拉韦、地塞米松、布地奈德、托珠单抗、巴瑞替尼、索托维单抗、康复期血浆、俯卧位和抗凝治疗。观察指标包括病毒载量、病毒标志物、无呼吸机天数或临床改善情况。
检索共发现302篇文章,52篇符合纳入标准。羟氯喹、地塞米松和瑞德西韦在老年COVID-19患者中显示出更多的副作用或无效。法匹拉韦、巴瑞替尼和支持性治疗显示病毒载量降低且临床症状改善。关于托珠单抗、康复期血浆和抗凝治疗在降低死亡率、无呼吸机天数和临床改善方面的证据存在矛盾。此外,由于索托维单抗和布地奈德治疗的正在进行的试验,证据有限且缺乏数据。
目前尚无已知药物可有效预防接触病毒后的COVID-19感染。需要进一步研究以确保所审查的每种干预措施对老年人的安全性和有效性。