Tondo Pasquale, Pronzato Caterina, Risi Irene, D'Artavilla Lupo Nadia, Trentin Rossella, Arcovio Simona, Fanfulla Francesco
Respiratory Function and Sleep Medicine Unit, Istituti Clinici Scientifici Maugeri IRCCS, 27100 Pavia, Italy.
Department of Medical and Surgical Sciences, University of Foggia, 71122 Foggia, Italy.
J Clin Med. 2022 Jun 1;11(11):3157. doi: 10.3390/jcm11113157.
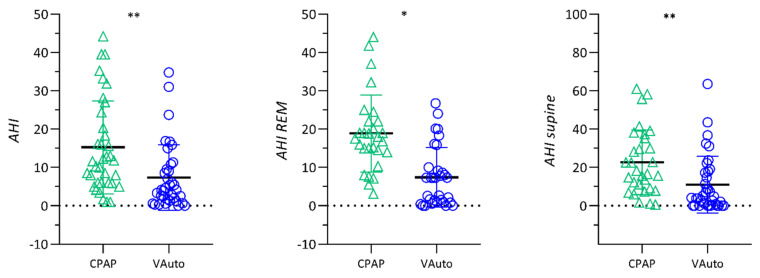
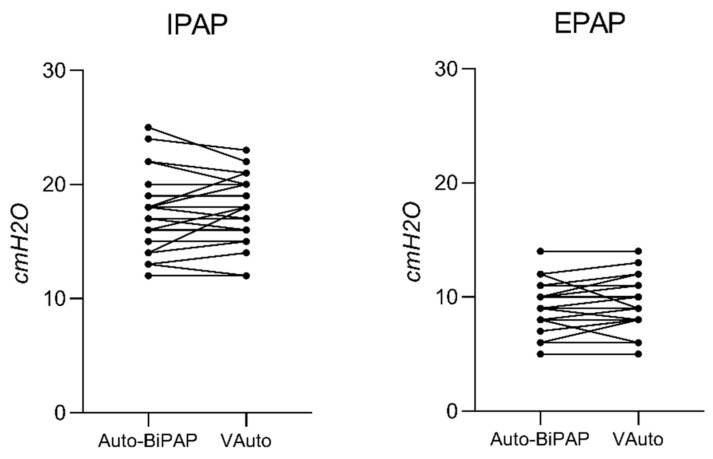
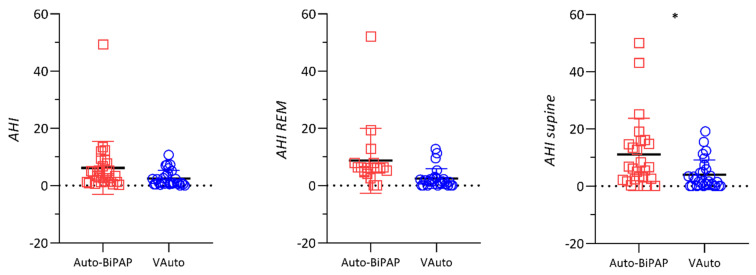
Background. Continuous positive airway pressure (CPAP) is considered the first-line treatment for patients with OSA, but Bilevel-PAP (BiPAP) therapy is a recognized option for noncompliant/unresponsive patients to CPAP. The present study was designed to evaluate the role of ResMed VAuto in the management of two different issues raised because of the Philips recall: the treatment of naïve noncompliant/unresponsive patients to CPAP (Group A) and the switch to VAuto for patients already on treatment with Philips Auto-BiPAP (Group B). Methods. Sixty-four patients who required auto-BiPAP treatment from August to December 2021 were included in the study. The efficacy of each mode of PAP therapy was compared between the two groups of patients. Results. Group A showed a statistically significant improvement in the apnea−hypopnea index (AHI) (7.4 ± 8.5 events·h−1 vs. 15.2 ± 12.1 events·h−1, p < 0.001), and oxygen desaturation index (ODI) (9.4 ± 8.9 events·h−1 vs. 15.2 ± 8.8 events·h−1, p = 0.029) during VAuto in comparison to CPAP, respectively. Conversely, a similar trend was found for patients in Group B for global AHI, but a statistically significant reduction was just found in supine AHI and ODI. In group B, an AHI <5 events·h−1 was found in 89.3% during VAuto in comparison to 82.1% with Philips Auto-BiPAP (p = ns). The levels of IPAPmax and EPAPmin were not statistically different between the two devices (p = 0.69 and p = 0.36, respectively). Conclusion. Bilevel ventilation in VAuto mode is effective in the clinical management of two different issues derived from the Philips recall. The switching between two different auto-BiPAP devices can be performed easily and successfully.
背景。持续气道正压通气(CPAP)被认为是阻塞性睡眠呼吸暂停(OSA)患者的一线治疗方法,但双水平气道正压通气(BiPAP)治疗是CPAP治疗不依从/无反应患者的公认选择。本研究旨在评估瑞思迈VAuto在处理因飞利浦召回引发的两个不同问题中的作用:治疗初治的CPAP治疗不依从/无反应患者(A组),以及将已接受飞利浦自动BiPAP治疗的患者转换为VAuto治疗(B组)。方法。纳入2021年8月至12月期间需要自动BiPAP治疗的64例患者。比较两组患者每种PAP治疗模式的疗效。结果。与CPAP相比,A组在VAuto治疗期间的呼吸暂停低通气指数(AHI)(7.4±8.5次·小时−1 vs. 15.2±12.1次·小时−1,p<0.001)和氧饱和度下降指数(ODI)(9.4±8.9次·小时−1 vs. 15.2±8.8次·小时−1,p = 0.029)有统计学意义的改善。相反,B组患者的总体AHI有类似趋势,但仅在仰卧位AHI和ODI方面有统计学意义的降低。在B组中,VAuto治疗期间89.3%的患者AHI<5次·小时−1,而飞利浦自动BiPAP治疗时为82.1%(p = 无统计学差异)。两种设备之间的吸气正压最大值(IPAPmax)和呼气正压最小值(EPAPmin)水平无统计学差异(分别为p = 0.69和p = 0.36)。结论。VAuto模式下的双水平通气在临床处理飞利浦召回引发的两个不同问题中有效。两种不同的自动BiPAP设备之间的转换可以轻松且成功地进行。