Deng Yang, Gu Jun-Yuan, Li Xin, Tong Huan, Guo Si-Wei, Xu Bing, Li You, Zhang Bi-Kui, Li Ying, Huang Hai-Ying, Xiao Gui-Ying
Department of Pharmacy, The Third Hospital of Changsha, 176 Western Laodong Road, Tianxin District, Changsha, 410015, Hunan, People's Republic of China.
The Clinical Application Research Institute of Antibiotics in Changsha, Changsha, 410015, Hunan, China.
Infect Dis Ther. 2022 Aug;11(4):1591-1608. doi: 10.1007/s40121-022-00655-3. Epub 2022 Jun 11.
The correlation between total and free polymyxin B (PMB including PMB1 and PMB2) exposure in vivo and acute kidney injury (AKI) remains obscure. This study explores the relationships between plasma exposure of PMB1 and PMB2 and nephrotoxicity, and investigates the risk factors for PMB-induced acute kidney injury (AKI) in critically ill patients.
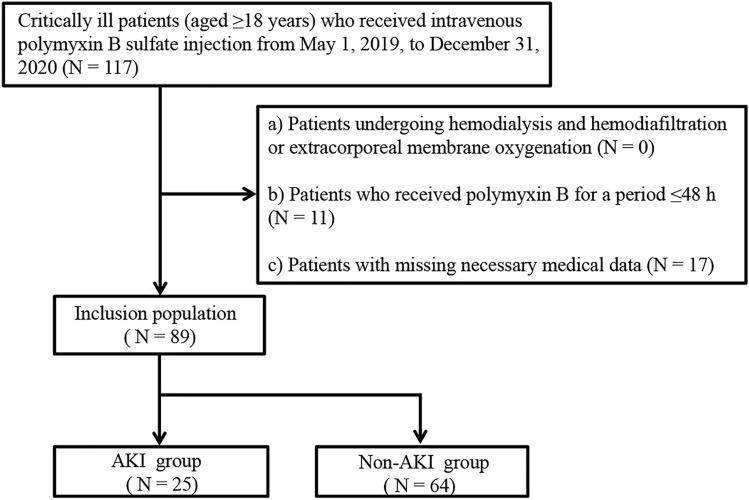
Critically ill patients who used PMB and met the criteria were enrolled. The total plasma concentration and plasma binding of PMB1 and PMB2 were analysed by liquid chromatography-tandem mass spectrometry and equilibrium dialysis.
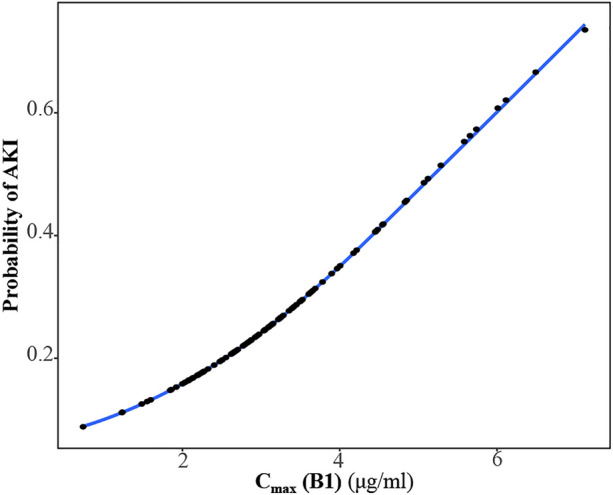
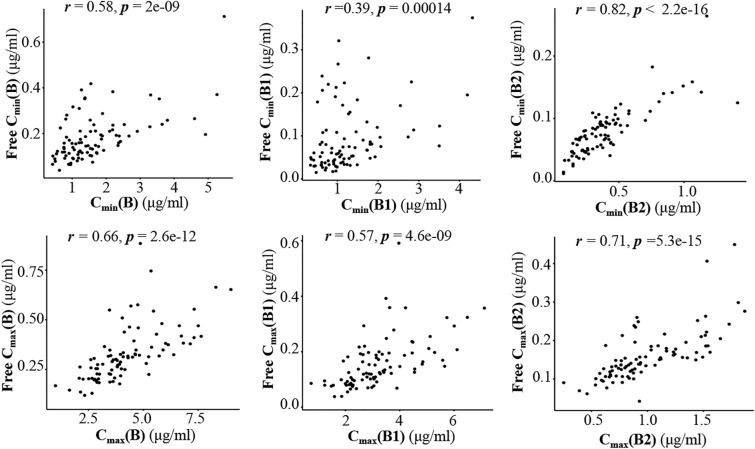
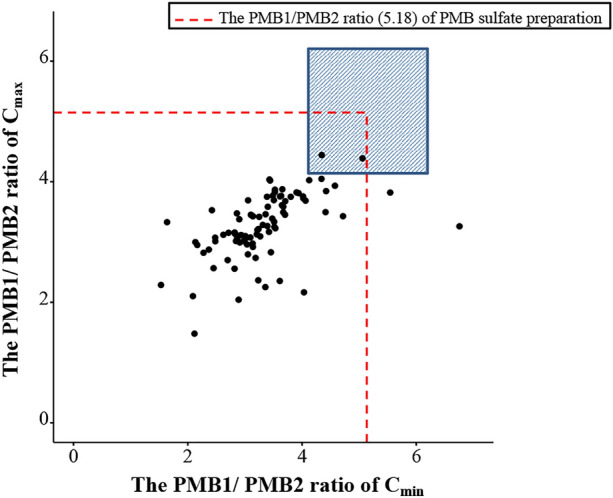
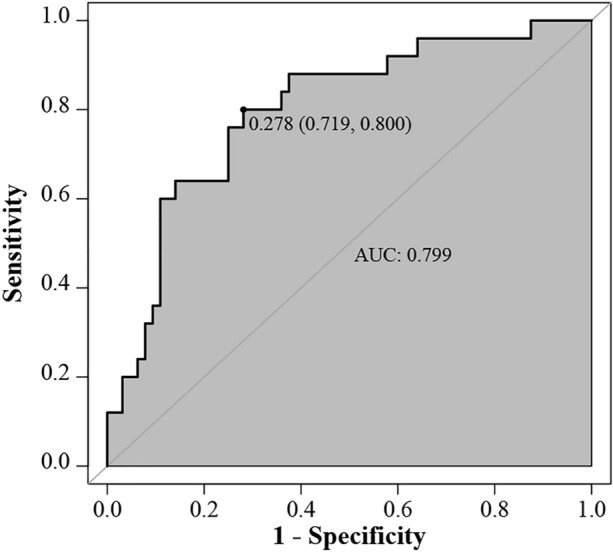
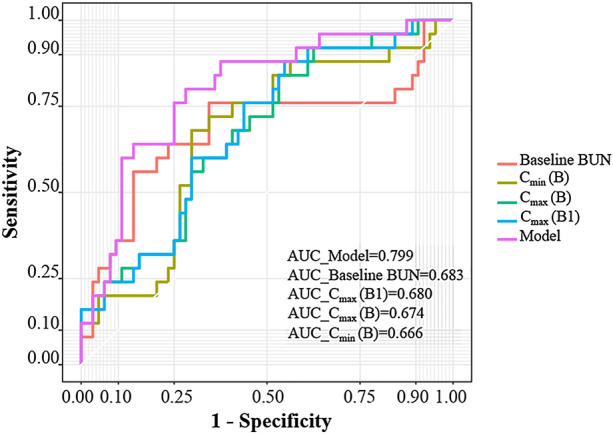
A total of 89 patients were finally included, and AKI developed in 28.1% of them. The peak concentration of PMB1 (C (B1)) (adjusted odds ratio (AOR) = 1.68, 95% CI 1.08-2.62, p = 0.023), baseline BUN level (AOR = 1.08, 95% CI 1.01-1.16, p = 0.039) and hypertension (AOR = 3.73, 95% CI 1.21-11.54, p = 0.022) were independent risk factors for PMB-induced AKI. The area under the ROC curve of the model was 0.799. When C (B1) was 5.23 μg/ml or more, the probability of AKI was higher than 50%. The ratio of PMB1/PMB2 decreased after PMB preparation entered into the body. The protein binding rate in critically ill patients indicated significant individual differences. Free C (B) and free C (B1) levels in the AKI group were significantly (p < 0.05) higher than those in the non-AKI group. Total and free concentrations of PMB in patients showed a positive correlation.
Both the ROC curve and logistic regression model showed that C (B1) was a good predictor for the probability of PMB-induced AKI. Early therapeutic drug monitoring (TDM) of PMB should be considered in critically ill patients. Compared with C (B), C (B) and C (B1) may be helpful for the early prediction of PMB-induced AKI in critically ill patients.
体内多粘菌素B(PMB,包括PMB1和PMB2)总量与游离量暴露与急性肾损伤(AKI)之间的相关性仍不明确。本研究探讨PMB1和PMB2的血浆暴露与肾毒性之间的关系,并调查重症患者中PMB诱导的急性肾损伤(AKI)的危险因素。
纳入使用PMB且符合标准的重症患者。采用液相色谱-串联质谱法和平衡透析法分析PMB1和PMB2的血浆总浓度及血浆结合率。
最终纳入89例患者,其中28.1%发生AKI。PMB1的峰浓度(C(B1))(调整优势比(AOR)=1.68,95%可信区间1.08 - 2.62,p = 0.023)、基线尿素氮水平(AOR = 1.08,95%可信区间1.01 - 1.16,p = 0.039)和高血压(AOR = 3.73,95%可信区间1.21 - 11.54,p = 0.022)是PMB诱导AKI的独立危险因素。该模型的ROC曲线下面积为0.799。当C(B1)≥5.23μg/ml时,AKI发生概率高于50%。PMB制剂进入体内后,PMB1/PMB2比值降低。重症患者的蛋白结合率存在显著个体差异。AKI组的游离C(B)和游离C(B1)水平显著高于非AKI组(p < 0.05)。患者体内PMB的总浓度和游离浓度呈正相关。
ROC曲线和逻辑回归模型均显示,C(B1)是PMB诱导AKI发生概率的良好预测指标。重症患者应考虑早期进行PMB的治疗药物监测(TDM)。与C(B)相比,C(B)和C(B1)可能有助于早期预测重症患者中PMB诱导的AKI。