Department of Respiratory Medicine, Nagoya University Graduate School of Medicine, 65 Tsurumai-cho, Showa-ku, Nagoya, 466-8550, Japan.
Department of Respiratory Medicine, Japanese Red Cross Aichi Medical Center Nagoya Daiichi Hospital, Nagoya, Japan.
BMC Cancer. 2022 Jun 14;22(1):654. doi: 10.1186/s12885-022-09741-8.
Osimertinib-the third-generation epidermal growth factor receptor (EGFR)-tyrosine kinase inhibitor (TKI)-has been widely used as a first-line treatment for patients with metastatic EGFR-mutant non-small cell lung cancer (NSCLC). Osimertinib demonstrated central nervous system activity in patients with brain metastasis; however, its efficacy against other distant metastatic organs, including bone and liver, remains unclear. Therefore, we retrospectively analyzed the clinical efficacy of osimertinib in these patients in comparison to other EGFR-TKIs.
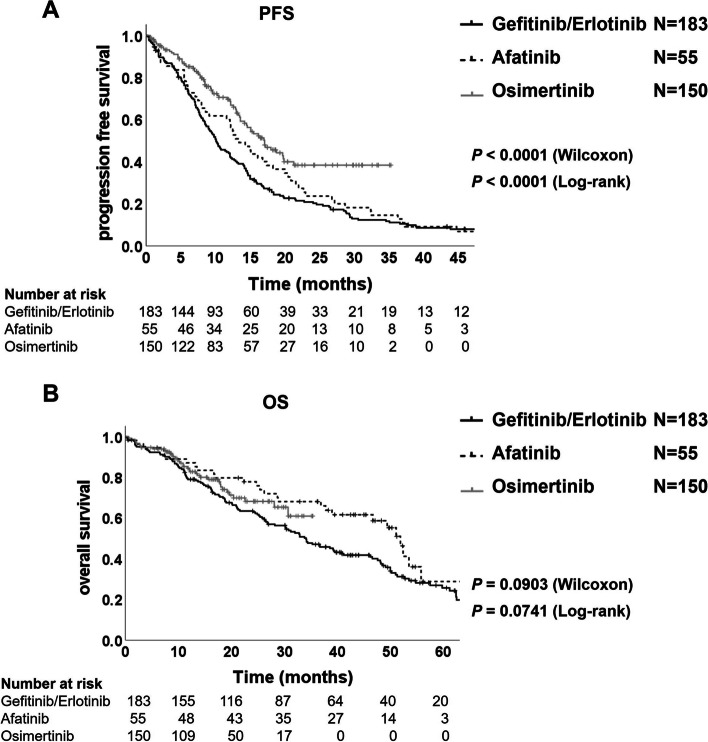
Clinical data of patients with advanced NSCLC receiving gefitinib/erlotinib (n = 183), afatinib (n = 55), or osimertinib (n = 150) at five medical institutions were retrospectively assessed for progression-free survival (PFS), overall survival (OS), and best overall response rate (ORR).
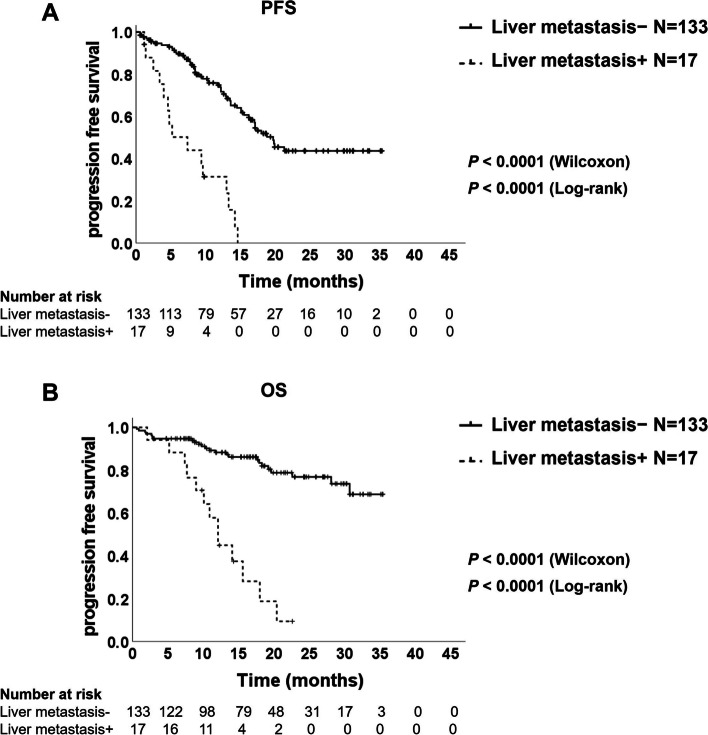
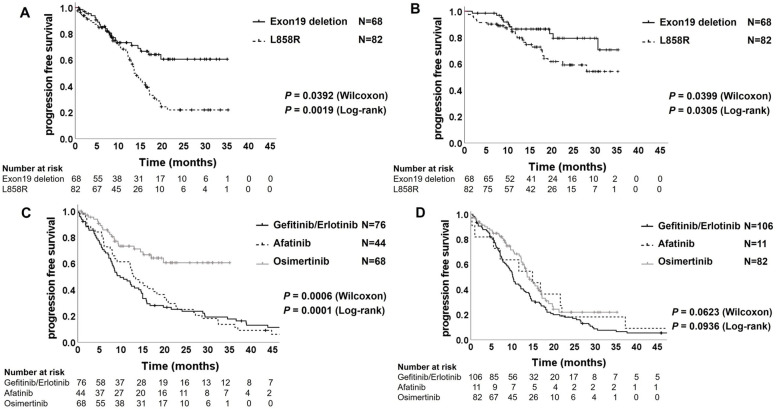
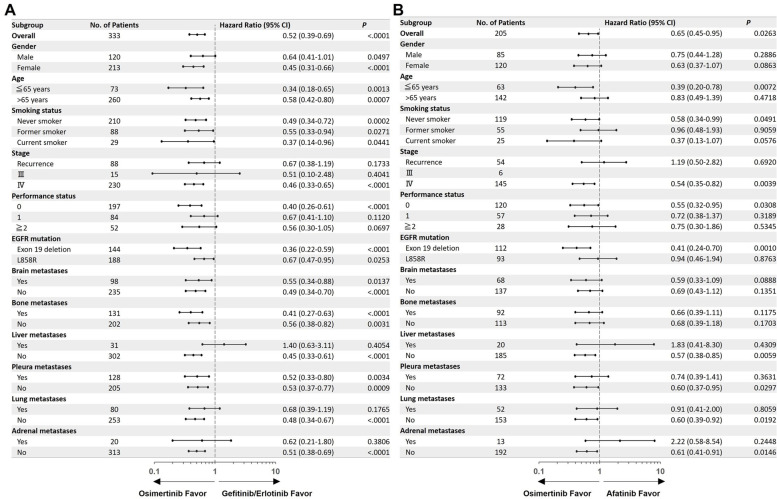
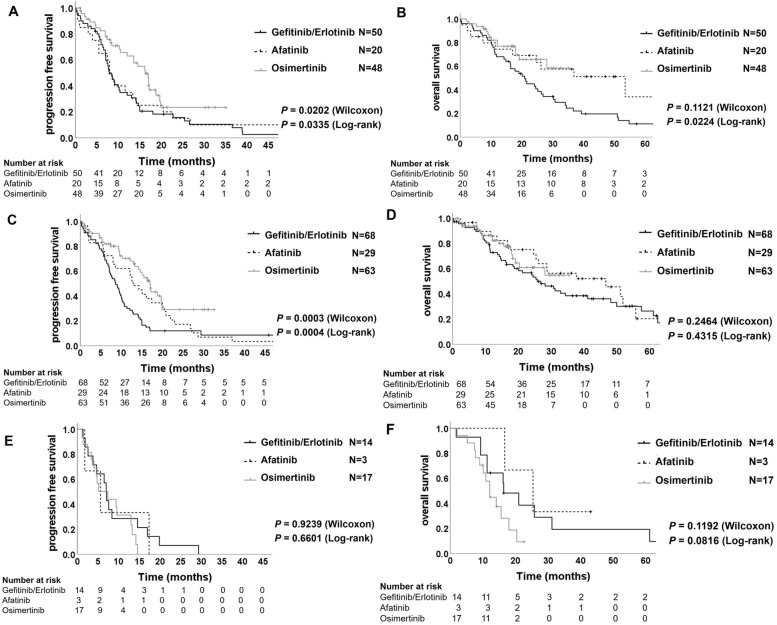
In univariate and multivariate analyses, most distant metastases, including the brain and bone, were unrelated to the therapeutic efficacy of osimertinib, although liver metastasis and L858R mutation were independently associated with shorter PFS. PFS and OS in patients with liver metastases were significantly shorter than those in patients without liver metastases (PFS: 7.4 vs. 19.7 months, OS: 12.1 months vs. not reached, respectively). Osimertinib provided significantly longer PFS in patients with brain or bone metastasis and exon 19 deletion than the other EGFR-TKIs. The PFS of patients with liver metastases was not significantly different among the three EGFR-TKI groups. Furthermore, the ORR of osimertinib in patients with liver metastases was significantly attenuated, and the effectiveness was similar to 1- or 2 -generation EGFR-TKIs.
Osimertinib provided better clinical benefits than 1- and 2-generation EGFR-TKIs for patients with EGFR-mutant NSCLC, particularly those with brain or bone metastases and exon 19 deletion; however, its efficacy against liver metastasis was remarkably attenuated. New therapeutic developments for patients with EGFR-mutant NSCLC with liver metastases are needed.
奥希替尼(第三代表皮生长因子受体 [EGFR] - 酪氨酸激酶抑制剂 [TKI])已广泛用作转移性 EGFR 突变型非小细胞肺癌(NSCLC)患者的一线治疗药物。奥希替尼在有脑转移的患者中显示出中枢神经系统活性;然而,其对包括骨和肝在内的其他远处转移器官的疗效尚不清楚。因此,我们回顾性分析了奥希替尼与其他 EGFR-TKI 相比在这些患者中的临床疗效。
回顾性评估了在五家医疗机构接受吉非替尼/厄洛替尼(n = 183)、阿法替尼(n = 55)或奥希替尼(n = 150)治疗的晚期 NSCLC 患者的无进展生存期(PFS)、总生存期(OS)和总缓解率(ORR)。
在单因素和多因素分析中,包括脑和骨在内的大多数远处转移与奥希替尼的疗效无关,尽管肝转移和 L858R 突变与较短的 PFS 独立相关。有肝转移的患者的 PFS 和 OS 明显短于无肝转移的患者(PFS:7.4 个月 vs. 19.7 个月,OS:12.1 个月 vs. 未达到)。奥希替尼为脑或骨转移和外显子 19 缺失的患者提供了显著更长的 PFS,优于其他 EGFR-TKI。有肝转移的患者在三种 EGFR-TKI 组之间,PFS 无显著差异。此外,奥希替尼治疗肝转移患者的 ORR 显著降低,疗效与 1 代或 2 代 EGFR-TKI 相似。
奥希替尼为 EGFR 突变型 NSCLC 患者提供了优于 1 代和 2 代 EGFR-TKI 的临床获益,尤其是脑或骨转移和外显子 19 缺失的患者;然而,其对肝转移的疗效显著降低。需要为 EGFR 突变型 NSCLC 伴肝转移的患者开发新的治疗方法。