Rush Medical College, Chicago, IL, USA.
Department of Surgery, Rush University Medical Center, Chicago, IL, USA.
Ann Surg Oncol. 2022 Nov;29(12):7652-7658. doi: 10.1245/s10434-022-12001-5. Epub 2022 Jun 24.
Despite improvements, disparities in breast cancer care have led to an inequitable distribution of treatment delays and worse outcomes among patients with breast cancer. This study aimed to quantify the contribution of mediators that may explain racial/ethnic disparities in breast cancer treatment delays.
We conducted a retrospective analysis of patients from the National Cancer Database with stage I-III breast cancer who underwent surgical resection. Mediation analyses estimated the extent to which racial/ethnic disparities in the distribution of patient characteristics account for racial/ethnic disparities in delayed treatment.
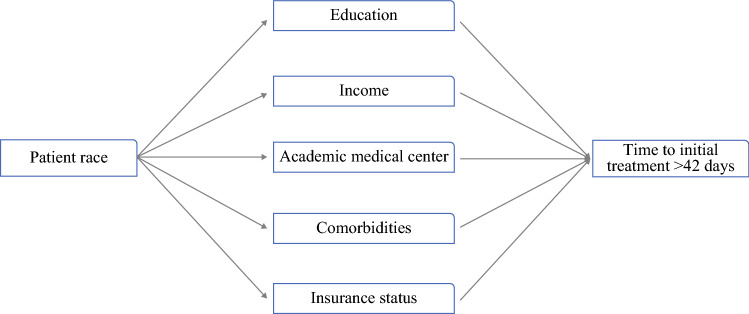
Of the 1,349,715 patients with breast cancer included, 10%, 5%, and 4% were Black, Hispanic, and other non-white race/ethnicity, respectively. Multivariable models showed that patients in these racial/ethnic groups had 73%, 81%, and 24% increased odds of having a treatment delay relative to white patients. Mediation analyses suggested that 15%, 19%, and 15% of the treatment delays among Black, Hispanic, and other non-white race/ethnicity patients, respectively, are explained by disparities in education, comorbidities, insurance, and facility type. Therefore, if these mediators had been distributed equally among all races/ethnicities, a reduction of 15-19% in the delayed treatment disparities experienced by minority patients would have been observed. Academic facility type was the factor that could yield the largest reduction in time to treatment disparities, contributing to 8-13% of racial/ethnic disparities.
Patients with breast cancer who identified as Black, Hispanic, and other non-white races/ethnicities are exposed to longer treatment delays relative to white patients. Efforts to equalize mediators could remove substantial portions of racial/ethnic disparities in delayed treatment.
尽管有所改善,但乳腺癌护理方面的差异导致治疗延迟在乳腺癌患者中的分布不均,治疗结果也更差。本研究旨在量化可能解释乳腺癌治疗延迟种族/民族差异的中介因素。
我们对接受手术切除的美国国家癌症数据库中 I-III 期乳腺癌患者进行了回顾性分析。中介分析估计了患者特征分布中的种族/民族差异在多大程度上导致了治疗延迟方面的种族/民族差异。
在纳入的 1349715 例乳腺癌患者中,分别有 10%、5%和 4%为黑人、西班牙裔和其他非白人种族/民族。多变量模型显示,这些种族/民族群体的患者接受治疗的延迟的可能性比白人患者分别高出 73%、81%和 24%。中介分析表明,黑人、西班牙裔和其他非白人种族/民族患者中分别有 15%、19%和 15%的治疗延迟可归因于教育、合并症、保险和医疗机构类型方面的差异。因此,如果这些中介因素在所有种族/民族中平等分布,少数民族患者经历的治疗延迟差异将减少 15-19%。学术医疗机构类型是可以最大程度减少治疗差异时间差异的因素,对种族/民族差异的贡献为 8-13%。
与白人患者相比,被认定为黑人、西班牙裔和其他非白人种族/民族的乳腺癌患者接受治疗的延迟时间更长。努力使中介因素均等化可以消除治疗延迟方面的大量种族/民族差异。