Department of Emergency, Xiangya Hospital, Central South University, Changsha, Hunan, People's Republic of China.
BMC Infect Dis. 2022 Jun 27;22(1):577. doi: 10.1186/s12879-022-07550-9.
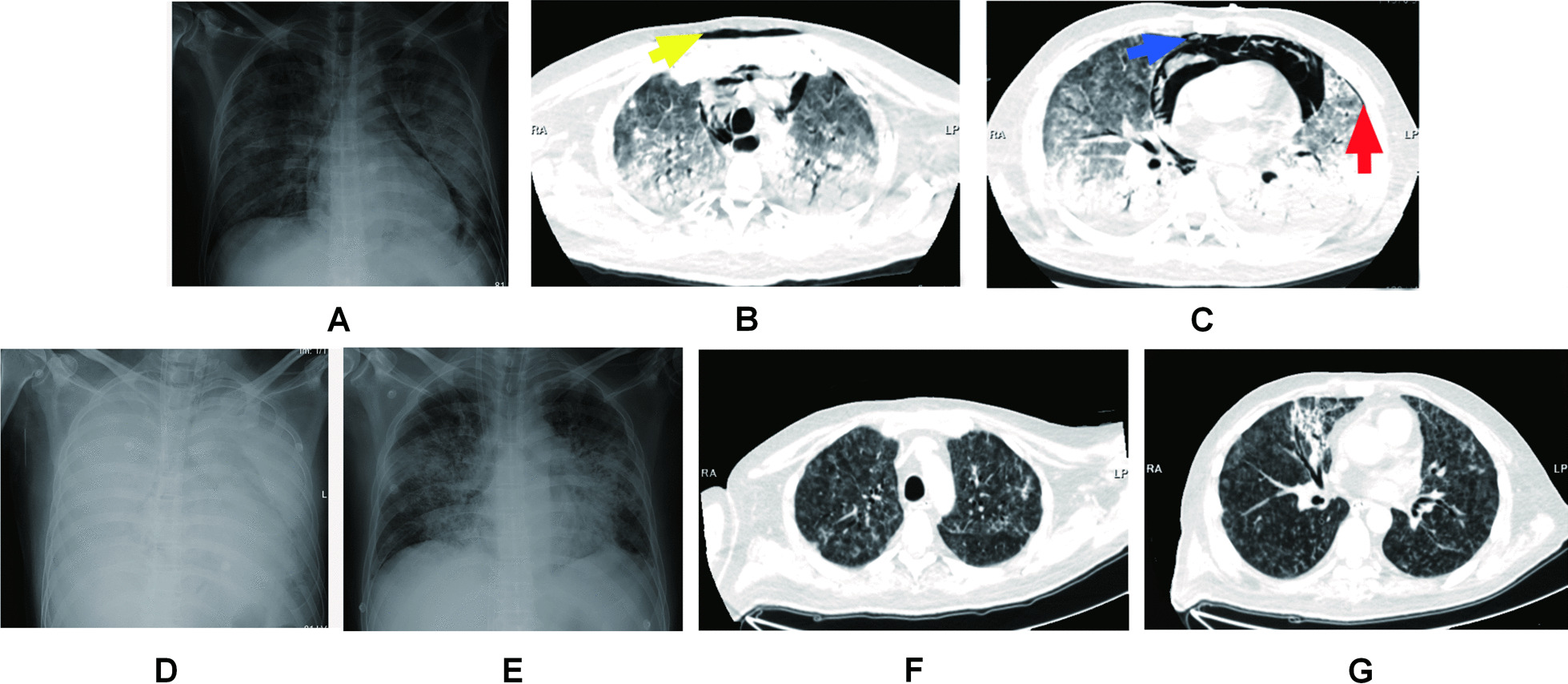
Pneumocystis jirovecii pneumonia (PJP) in an immunocompromised host is often associated with the Macklin effect, which can progress to spontaneous pneumomediastinum (SPM), subcutaneous emphysema (SCE), and pneumothorax (PNX). Diagnosing the causative organism of these conditions in non-HIV infected patients and treating hypoxemia while preventing further lung damage can be challenging. This study examines the case of a non-HIV infected male with SPM, SCE, and PNX secondary to severe Pneumocystis jirovecii (PJ) infection.
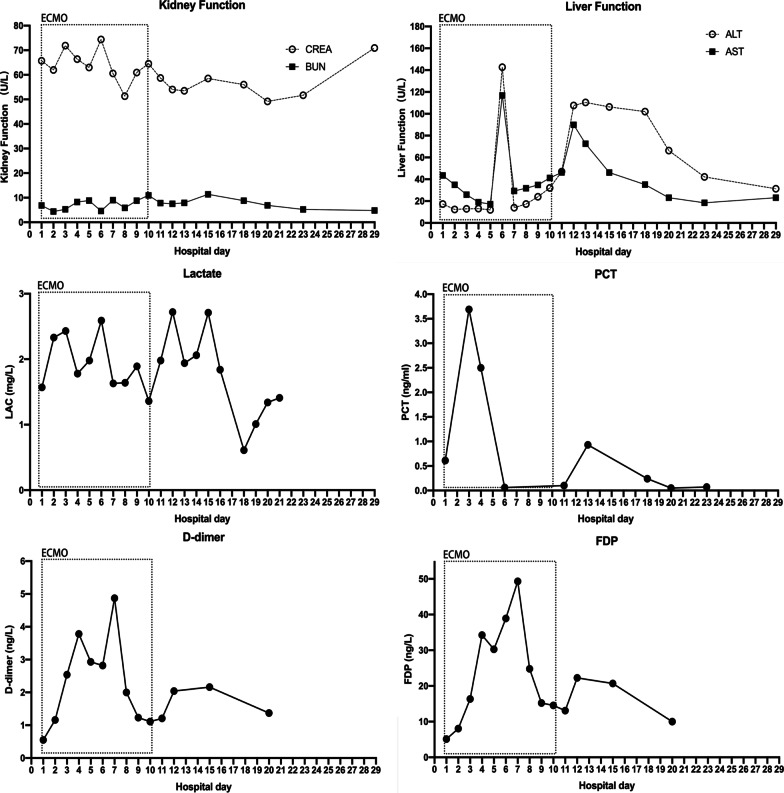
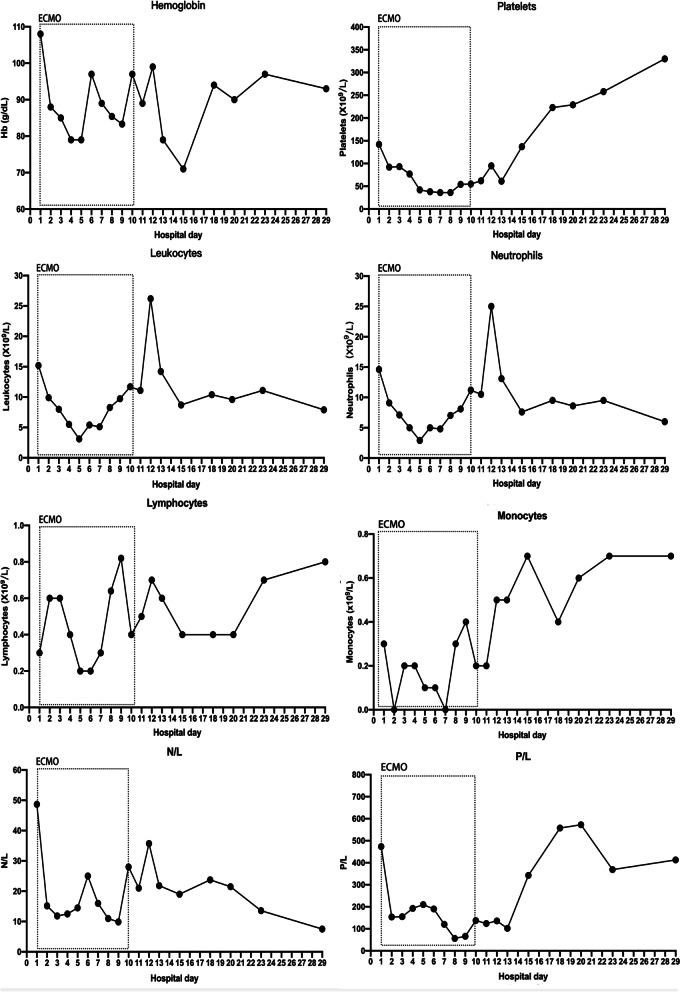
A 53-year-old male with pure red cell aplasia (PRCA) was admitted with fever, dry cough, and shortness of breath. His respiratory function progressively deteriorated due to the development of SPM, SCE, and PNX, eventually requiring endotracheal intubation and invasive ventilation. As a result of high pressure in his airways occasioned by lung recruitment maneuvers, his pulmonary parameters worsened, necessitating veno-venous (VV) extracorporeal membrane oxygenation (ECMO) therapy. The early initiation of VV-ECMO facilitated ultra-protective lung ventilation and prevented the progression of SPM, SCE, and PNX. Traditional diagnostic assays were unrevealing, whereupon the patient resorted to the metagenomic next-generation sequencing technology for uncovering potential pathogens. Consequently, we detected a significantly higher infection by PJ in the patient's bronchoscopy lavage fluid. Finally, the patient was successfully treated with appropriate antimicrobials and was decannulated after nine days of ECMO support.
SPM, SCE, and PNX are rare clinical manifestations of PJP. However, they can be considered as poor prognostic factors of the infection. Physicians should, therefore, be alert to the possibility of PJP in immunocompromised patients.
免疫功能低下宿主的卡氏肺孢子菌肺炎(PJP)常与麦金效应相关,可进展为自发性纵隔气肿(SPM)、皮下气肿(SCE)和气胸(PNX)。在非 HIV 感染患者中诊断这些疾病的致病病原体并在治疗低氧血症的同时预防进一步的肺损伤可能具有挑战性。本研究检查了一例非 HIV 感染男性患者,因严重卡氏肺孢子菌(PJ)感染而继发 SPM、SCE 和 PNX。
一名 53 岁男性患有纯红细胞再生障碍性贫血(PRCA),因发热、干咳和呼吸急促入院。由于 SPM、SCE 和 PNX 的发展,他的呼吸功能逐渐恶化,最终需要进行气管插管和有创通气。由于肺复张手法引起气道高压,他的肺部参数恶化,需要进行静脉-静脉(VV)体外膜氧合(ECMO)治疗。VV-ECMO 的早期启动促进了超保护性肺通气,并防止了 SPM、SCE 和 PNX 的进展。传统的诊断检测方法没有发现结果,随后患者采用宏基因组下一代测序技术来发现潜在的病原体。因此,我们在患者的支气管镜灌洗液中检测到 PJ 的感染明显更高。最终,患者在接受适当的抗菌药物治疗后成功康复,并在 ECMO 支持九天后拔管。
SPM、SCE 和 PNX 是 PJP 的罕见临床表现。然而,它们可以被认为是感染的不良预后因素。因此,医生应该警惕免疫功能低下患者中发生 PJP 的可能性。