Faculty of Health and Life Sciences, Oxford Brookes University Faculty of Health and Life Sciences, Oxford, UK
Faculty of Health and Life Sciences, Oxford Brookes University, Oxford, UK.
BMJ Open. 2022 Jul 5;12(7):e056517. doi: 10.1136/bmjopen-2021-056517.
Water immersion during labour using a birth pool to achieve relaxation and pain relief during the first and possibly part of the second stage of labour is an increasingly popular care option in several countries. It is used particularly by healthy women who experience a straightforward pregnancy, labour spontaneously at term gestation and plan to give birth in a midwifery led care setting. More women are also choosing to give birth in water. There is debate about the safety of intrapartum water immersion, particularly waterbirth. We synthesised the evidence that compared the effect of water immersion during labour or waterbirth on intrapartum interventions and outcomes to standard care with no water immersion. A secondary objective was to synthesise data relating to clinical care practices and birth settings that women experience who immerse in water and women who do not.
Systematic review and meta-analysis.
A search was conducted using CINAHL, Medline, Embase, BioMed Central and PsycINFO during March 2020 and was replicated in May 2021.
Primary quantitative studies published in 2000 or later, examining maternal or neonatal interventions and outcomes using the birthing pool for labour and/or birth.
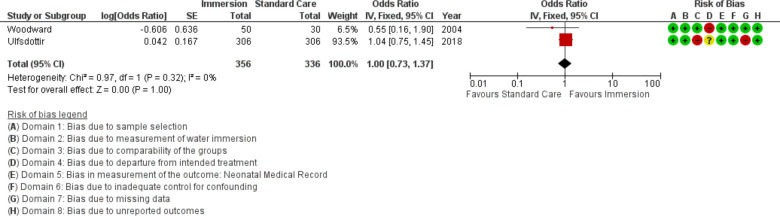
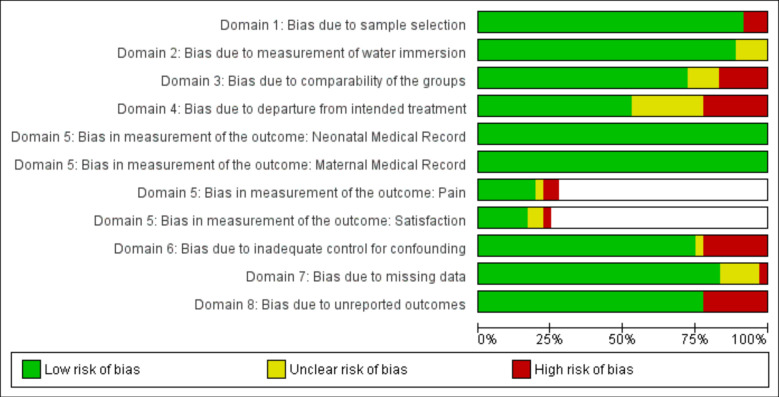
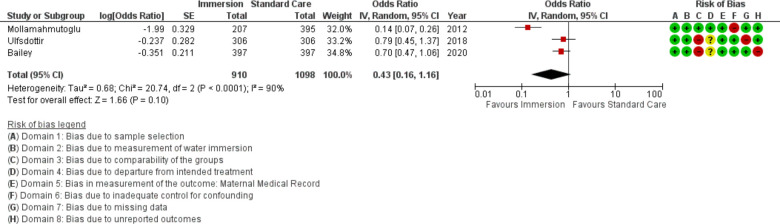
Full-text screening was undertaken independently against inclusion/exclusion criteria in two pairs. Risk of bias assessment included review of seven domains based on the Robbins-I Risk of Bias Tool. All outcomes were summarised using an OR and 95% CI. All calculations were conducted in Comprehensive Meta-Analysis V.3, using the inverse variance method. Results of individual studies were converted to log OR and SE for synthesis. Fixed effects models were used when I was less than 50%, otherwise random effects models were used. The fail-safe N estimates were calculated to determine the number of studies necessary to change the estimates. Begg's test and Egger's regression risk assessed risk of bias across studies. Trim-and-fill analysis was used to estimate the magnitude of effect of the bias. Meta-regression was completed when at least 10 studies provided data for an outcome.
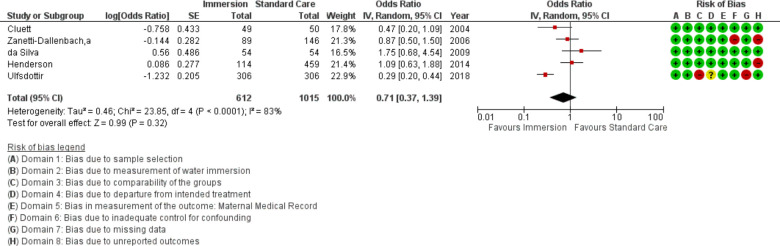
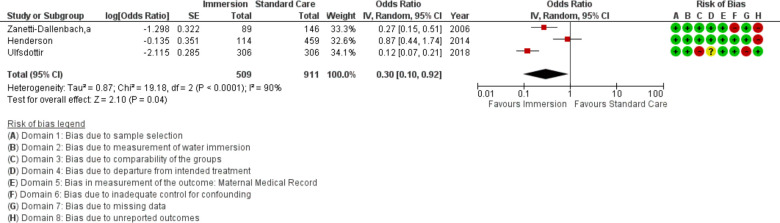
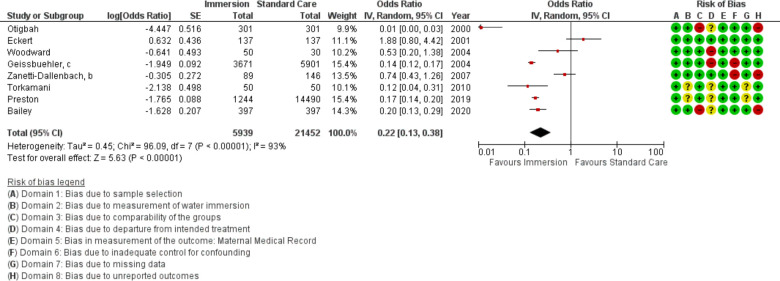
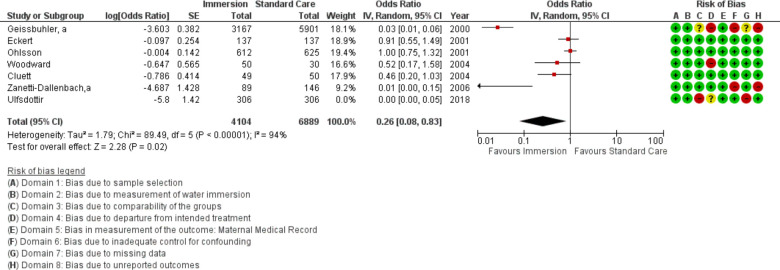
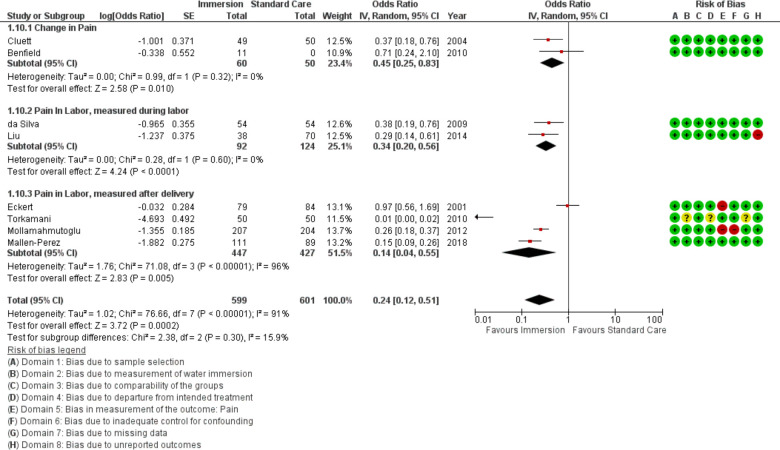
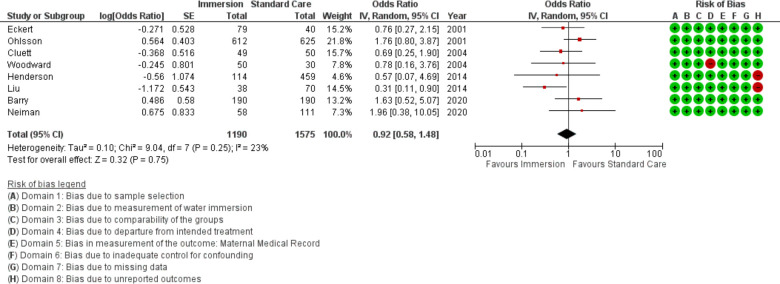
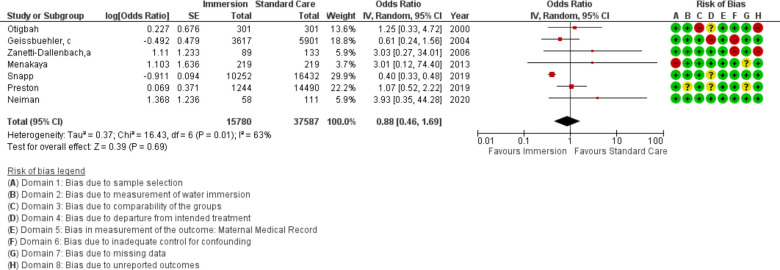
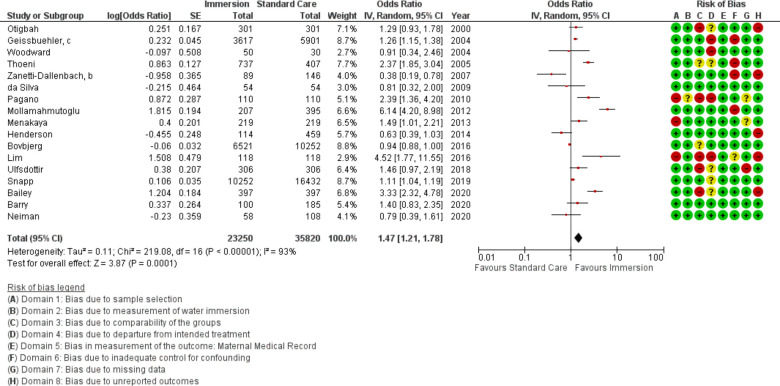
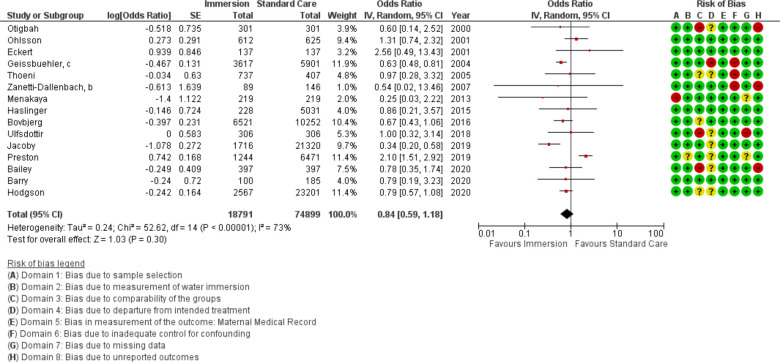
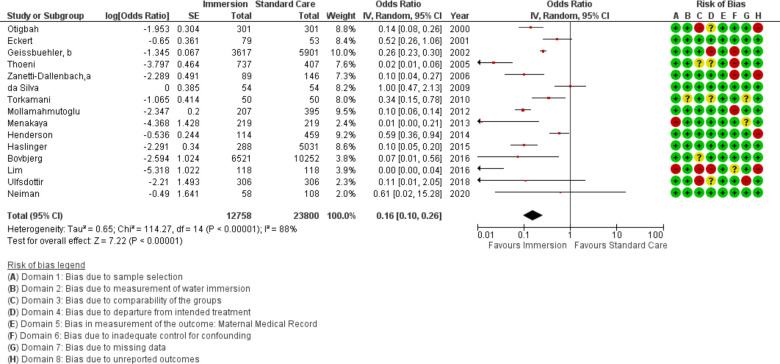
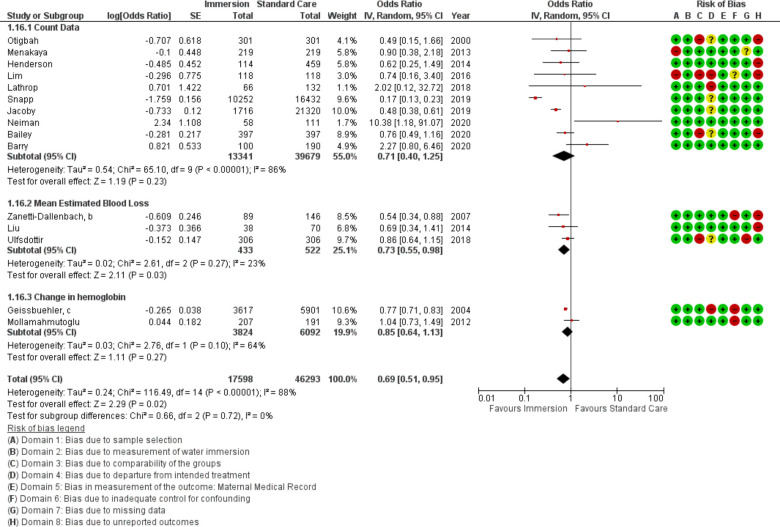
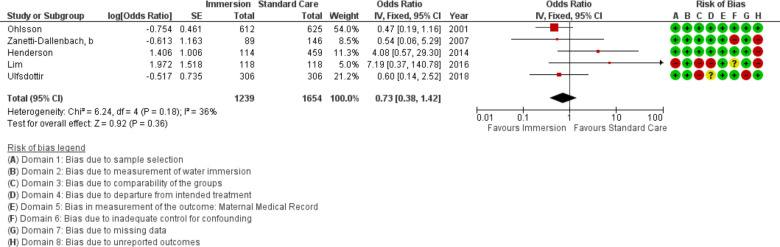
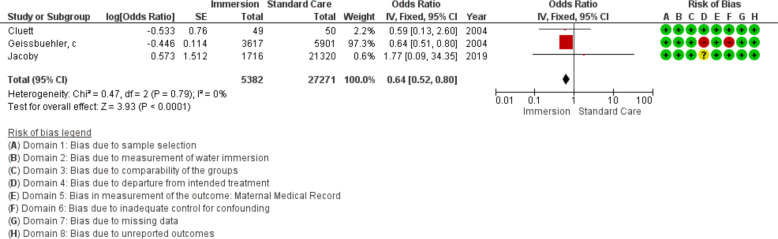
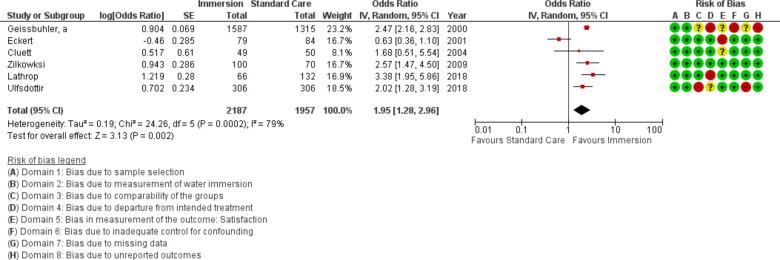
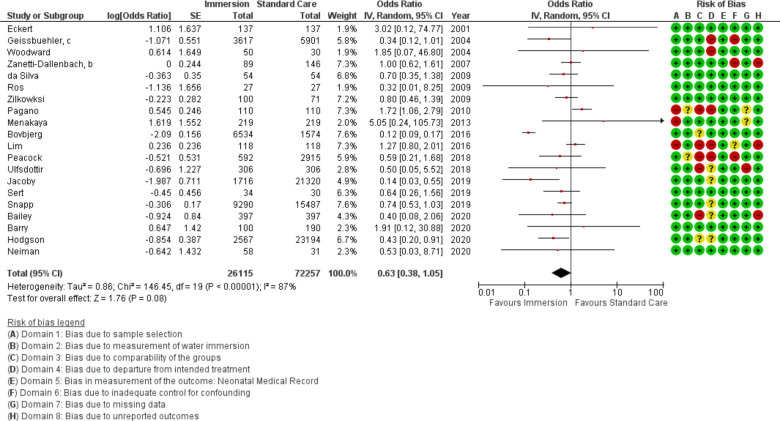
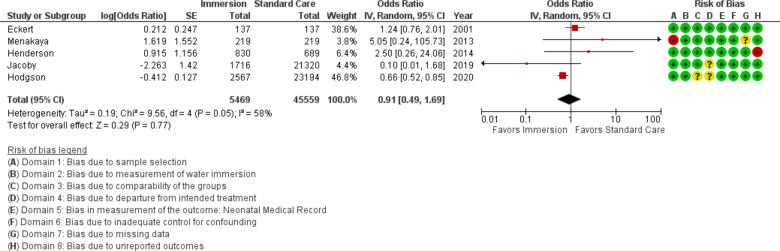
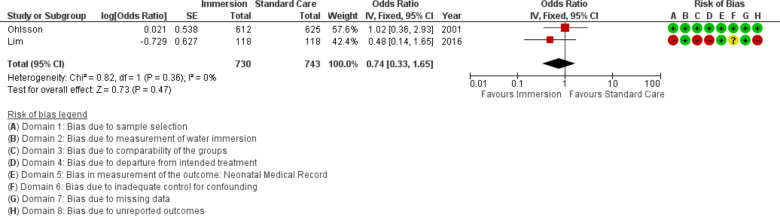
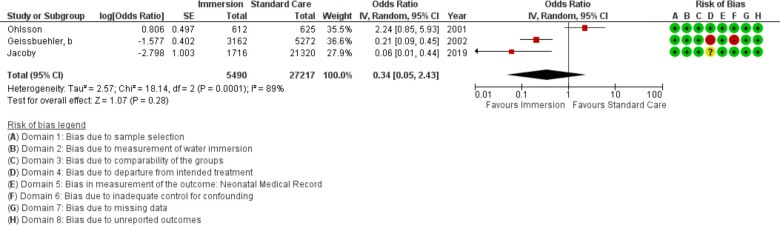
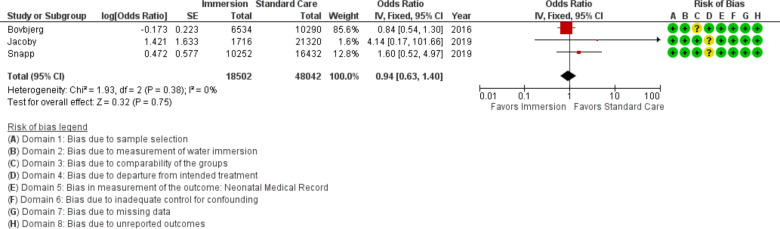
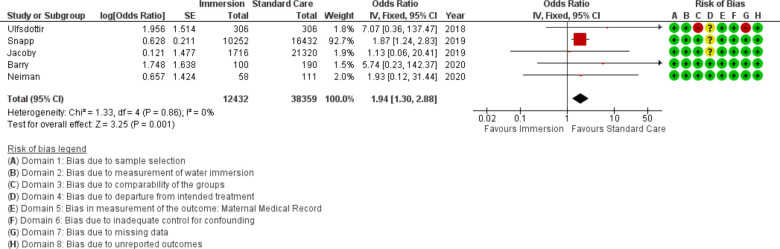
We included 36 studies in the review, (N=157 546 participants). Thirty-one studies were conducted in an obstetric unit setting (n=70 393), four studies were conducted in midwife led settings (n=61 385) and one study was a mixed setting (OU and homebirth) (n=25 768). Midwife led settings included planned home and freestanding midwifery unit (k=1), alongside midwifery units (k=1), planned homebirth (k=1), a freestanding midwifery unit and an alongside midwifery unit (k=1) and an alongside midwifery unit (k=1). For water immersion, 25 studies involved women who planned to have/had a waterbirth (n=151 742), seven involved water immersion for labour only (1901), three studies reported on water immersion during labour and waterbirth (n=3688) and one study was unclear about the timing of water immersion (n=215).Water immersion significantly reduced use of epidural (k=7, n=10 993; OR 0.17 95% CI 0.05 to 0.56), injected opioids (k=8, n=27 391; OR 0.22 95% CI 0.13 to 0.38), episiotomy (k=15, n=36 558; OR 0.16; 95% CI 0.10 to 0.27), maternal pain (k=8, n=1200; OR 0.24 95% CI 0.12 to 0.51) and postpartum haemorrhage (k=15, n=63 891; OR 0.69 95% CI 0.51 to 0.95). There was an increase in maternal satisfaction (k=6, n=4144; OR 1.95 95% CI 1.28 to 2.96) and odds of an intact perineum (k=17, n=59 070; OR 1.48; 95% CI 1.21 to 1.79) with water immersion. Waterbirth was associated with increased odds of cord avulsion (OR 1.94 95% CI 1.30 to 2.88), although the absolute risk remained low (4.3 per 1000 vs 1.3 per 1000). There were no differences in any other identified neonatal outcomes.
This review endorses previous reviews showing clear benefits resulting from intrapartum water immersion for healthy women and their newborns. While most included studies were conducted in obstetric units, to enable the identification of best practice regarding water immersion, future birthing pool research should integrate factors that are known to influence intrapartum interventions and outcomes. These include maternal parity, the care model, care practices and birth setting.
CRD42019147001.
在分娩过程中使用分娩池进行水中浸泡,以在第一产程和可能的第二产程的部分阶段实现放松和缓解疼痛,这是在多个国家越来越受欢迎的护理选择。它特别适用于经历简单妊娠、足月自然分娩并计划在助产士主导的护理环境中分娩的健康女性。越来越多的女性也选择在水中分娩。关于产时水中浸泡的安全性,特别是水中分娩,存在争议。我们综合了比较水中浸泡分娩或水中分娩与无水中浸泡的标准护理对产时干预措施和结局影响的证据。次要目标是综合与女性水中浸泡和不水中浸泡的临床护理实践和分娩环境相关的数据。
系统评价和荟萃分析。
2020 年 3 月使用 CINAHL、Medline、Embase、BioMed Central 和 PsycINFO 进行了搜索,并于 2021 年 5 月进行了复制。
发表于 2000 年或之后的主要定量研究,使用分娩池检查产妇或新生儿干预措施和结局。
在两名配对人员中,根据纳入/排除标准对全文进行筛选。风险偏倚评估包括基于 Robbins-I 风险偏倚工具的七个领域的审查。所有结局均使用 OR 和 95%CI 进行总结。所有计算均在 Comprehensive Meta-Analysis V.3 中使用逆方差法进行。个体研究的结果转换为 logOR 和 SE 以进行综合分析。当 I 小于 50%时使用固定效应模型,否则使用随机效应模型。失效安全 N 估计值用于确定改变估计所需的研究数量。Begg 检验和 Egger 回归风险评估了研究之间的偏倚风险。使用修剪和填充分析估计偏倚的效应大小。当至少有 10 项研究提供了某个结局的数据时,完成了荟萃回归分析。
我们对 36 项研究进行了综述,(N=157546 名参与者)。31 项研究在产科病房环境中进行(n=70393),4 项研究在助产士主导的环境中进行(n=61385),1 项研究在混合环境中进行(OU 和家庭分娩)(n=25768)。助产士主导的环境包括计划的家庭和独立助产士单位(k=1)、独立助产士单位(k=1)、计划的家庭分娩(k=1)、独立助产士单位和独立助产士单位(k=1)以及独立助产士单位(k=1)。对于水中浸泡,25 项研究涉及计划进行/已经进行水中分娩的女性(n=151742),7 项研究涉及仅用于分娩的水中浸泡(n=1901),3 项研究报告了分娩期间和水中分娩时的水中浸泡(n=3688),1 项研究对水中浸泡的时间不清楚(n=215)。水中浸泡显著降低了硬膜外麻醉(k=7,n=10993;OR 0.17,95%CI 0.05 至 0.56)、注射类阿片(k=8,n=27391;OR 0.22,95%CI 0.13 至 0.38)、会阴切开术(k=15,n=36558;OR 0.16,95%CI 0.10 至 0.27)、产妇疼痛(k=8,n=1200;OR 0.24,95%CI 0.12 至 0.51)和产后出血(k=15,n=63891;OR 0.69,95%CI 0.51 至 0.95)。水中浸泡增加了产妇满意度(k=6,n=4144;OR 1.95,95%CI 1.28 至 2.96)和完整会阴的可能性(k=17,n=59070;OR 1.48,95%CI 1.21 至 1.79)。水中分娩与脐带脱垂的几率增加(OR 1.94,95%CI 1.30 至 2.88)相关,尽管绝对风险仍然较低(每 1000 例 4.3 例与每 1000 例 1.3 例)。没有其他新生儿结局存在差异。
本综述支持以前的综述结果,即产时水中浸泡对健康女性及其新生儿有明显益处。尽管大多数纳入的研究是在产科病房进行的,但为了确定水中浸泡的最佳实践,未来的分娩池研究应整合已知会影响产时干预措施和结局的因素。这些因素包括产妇的产次、护理模式、护理实践和分娩环境。
CRD42019147001。