Department of Immunology, University of Toronto, Toronto, ON, Canada.
Schroeder Arthritis Institute, Krembil Research Institute, University Health Network, Toronto, ON, Canada.
Front Immunol. 2022 Jun 30;13:886442. doi: 10.3389/fimmu.2022.886442. eCollection 2022.
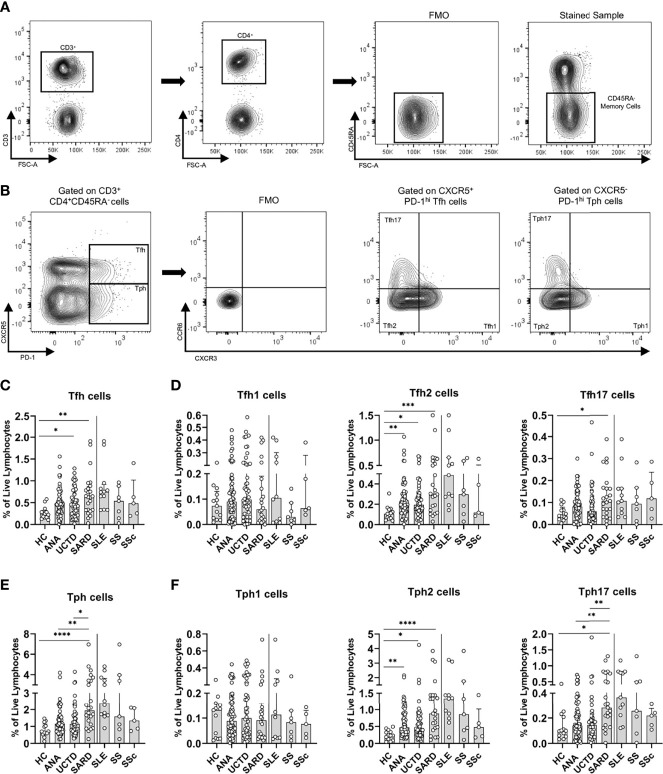
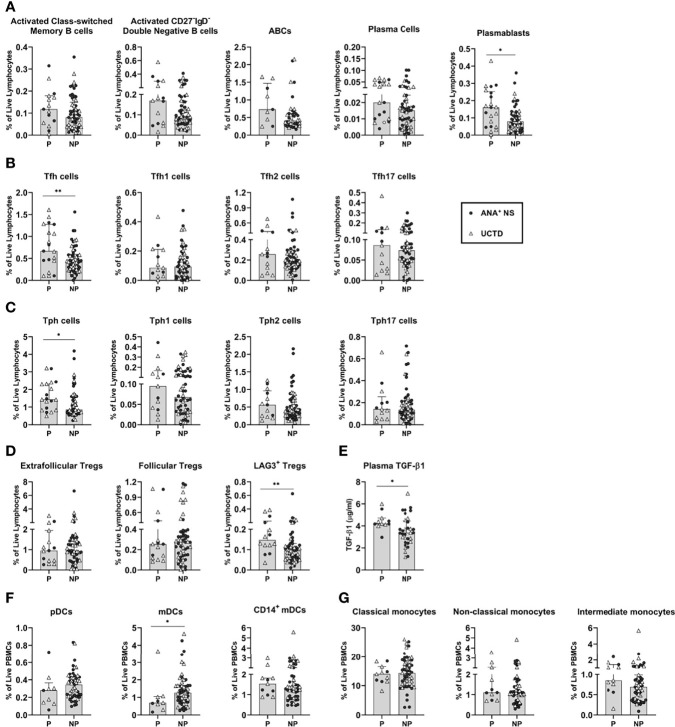
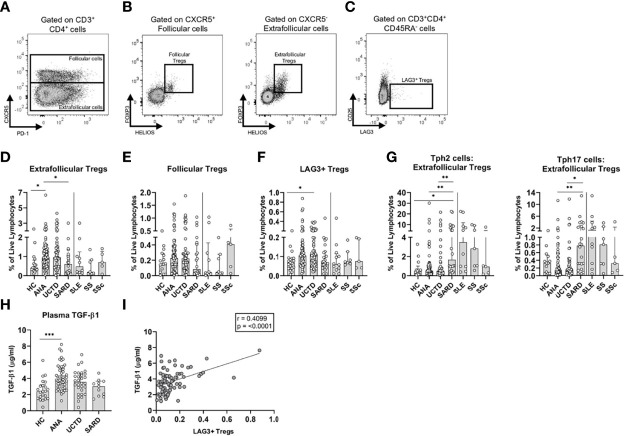
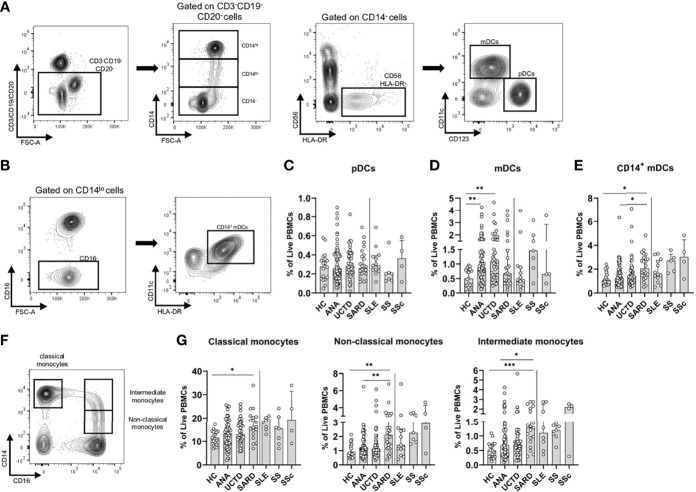
Systemic Autoimmune Rheumatic Diseases (SARDs) are characterized by the production of anti-nuclear antibodies (ANAs). ANAs are also seen in healthy individuals and can be detected years before disease onset in SARD. Both the immunological changes that promote development of clinical symptoms in SARD and those that prevent autoimmunity in asymptomatic ANA individuals (ANA NS) remain largely unexplored. To address this question, we used flow cytometry to examine peripheral blood immune populations in ANA individuals, with and without SARD, including 20 individuals who subsequently demonstrated symptom progression. Several immune populations were expanded in ANA individuals with and without SARD, as compared with ANA healthy controls, particularly follicular and peripheral T helper, and antibody-producing B cell subsets. In ANA NS individuals, there were significant increases in T regulatory subsets and TGF-ß1 that normalized in SARD patients, whereas in SARD patients there were increases in Th2 and Th17 helper cell levels as compared with ANA NS individuals, resulting in a shift in the balance between inflammatory and regulatory T cell subsets. Patients with SARD also had increases in the proportion of pro-inflammatory innate immune cell populations, such as CD14 myeloid dendritic cells, and intermediate and non-classical monocytes, as compared to ANA NS individuals. When comparing ANA individuals without SARD who progressed clinically over the subsequent 2 years with those who did not, we found that progressors had significantly increased T and B cell activation, as well as increased levels of LAG3 T regulatory cells and TGF-ß1. Collectively, our findings suggest that active immunoregulation prevents clinical autoimmunity in ANA NS and that this becomes impaired in patients who progress to SARD, resulting in an imbalance favoring inflammation.
系统性自身免疫性风湿病 (SARD) 的特征是产生抗核抗体 (ANA)。健康个体中也可见到 ANA,并且在 SARD 发病前数年即可检测到。在 SARD 中,促进临床症状发展的免疫变化和防止无症状 ANA 个体 (ANA NS) 发生自身免疫的免疫变化在很大程度上仍未得到探索。为了解决这个问题,我们使用流式细胞术检查了有和没有 SARD 的 ANA 个体的外周血免疫群体,包括 20 名随后表现出症状进展的个体。与 ANA 健康对照相比,ANA 个体和有 SARD 的个体中几种免疫群体都有扩张,特别是滤泡和外周辅助性 T 细胞以及产生抗体的 B 细胞亚群。在 ANA NS 个体中,T 调节亚群和 TGF-β1 显著增加,并在 SARD 患者中恢复正常,而与 ANA NS 个体相比,SARD 患者中的 Th2 和 Th17 辅助细胞水平增加,导致炎症和调节性 T 细胞亚群之间的平衡发生转变。与 ANA NS 个体相比,SARD 患者还增加了促炎先天免疫细胞群体的比例,如 CD14 髓样树突状细胞以及中间和非经典单核细胞。在比较随后 2 年内临床进展的无 SARD 的 ANA 个体与未进展的个体时,我们发现进展者的 T 和 B 细胞激活显著增加,以及 LAG3 T 调节细胞和 TGF-β1 水平增加。总的来说,我们的发现表明,活跃的免疫调节可防止 ANA NS 发生临床自身免疫,而在进展为 SARD 的患者中,这种调节会受损,导致炎症倾向的失衡。