Division of Infectious Diseases, Geneva University Hospital and Faculty of Medicine, University of Geneva, Geneva, Switzerland.
Division of Infection Control, Geneva University Hospital and Faculty of Medicine, University of Geneva, Geneva, Switzerland.
Lancet Infect Dis. 2022 Oct;22(10):1493-1502. doi: 10.1016/S1473-3099(22)00308-5. Epub 2022 Jul 20.
Computerised decision-support systems (CDSSs) for antibiotic stewardship could help to assist physicians in the appropriate prescribing of antibiotics. However, high-quality evidence for their effect on the quantity and quality of antibiotic use remains scarce. The aim of our study was to assess whether a computerised decision support for antimicrobial stewardship combined with feedback on prescribing indicators can reduce antimicrobial prescriptions for adults admitted to hospital.
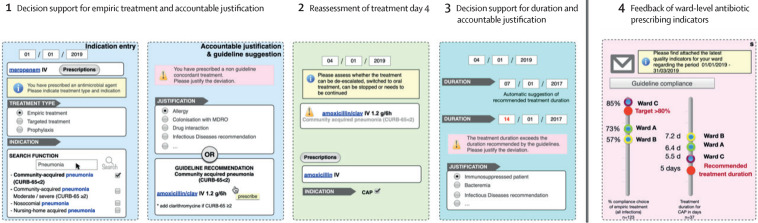
The Computerised Antibiotic Stewardship Study (COMPASS) was a multicentre, cluster-randomised, parallel-group, open-label superiority trial that aimed to assess whether a multimodal computerised antibiotic-stewardship intervention is effective in reducing antibiotic use for adults admitted to hospital. After pairwise matching, 24 wards in three Swiss tertiary-care and secondary-care hospitals were randomised (1:1) to the CDSS intervention or to standard antibiotic stewardship measures using an online random sequence generator. The multimodal intervention consisted of a CDSS providing support for choice, duration, and re-evaluation of antimicrobial therapy, and feedback on antimicrobial prescribing quality. The primary outcome was overall systemic antibiotic use measured in days of therapy per admission, using adjusted-hurdle negative-binomial mixed-effects models. The analysis was done by intention to treat and per protocol. The study was registered with ClinicalTrials.gov (identifier NCT03120975).
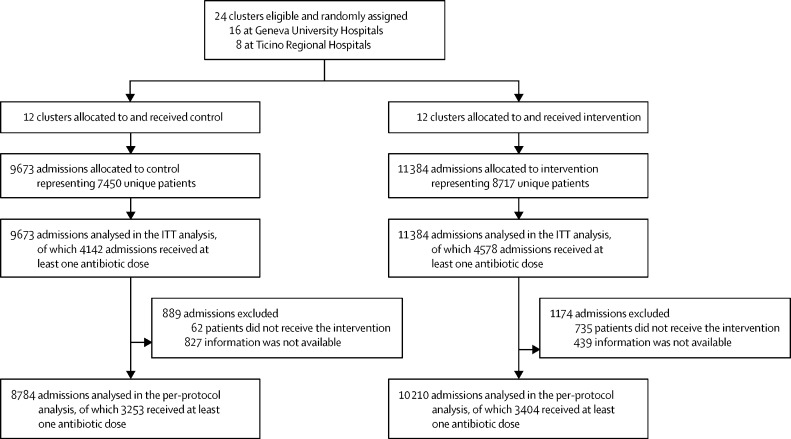
24 clusters (16 at Geneva University Hospitals and eight at Ticino Regional Hospitals) were eligible and randomly assigned to control or intervention between Oct 1, 2018, and Dec 31, 2019. Overall, 4578 (40·2%) of 11 384 admissions received antibiotic therapy in the intervention group and 4142 (42·8%) of 9673 in the control group. The unadjusted overall mean days of therapy per admission was slightly lower in the intervention group than in the control group (3·2 days of therapy per admission, SD 6·2, vs 3·5 days of therapy per admission, SD 6·8; p<0·0001), and was similar among patients receiving antibiotics (7·9 days of therapy per admission, SD 7·6, vs 8·1 days of therapy per admission, SD 8·4; p=0·50). After adjusting for confounders, there was no statistically significant difference between groups for the odds of an admission receiving antibiotics (odds ratio [OR] for intervention vs control 1·12, 95% CI 0·94-1·33). For admissions with antibiotic exposure, days of therapy per admission were also similar (incidence rate ratio 0·98, 95% CI 0·90-1·07). Overall, the CDSS was used at least once in 3466 (75·7%) of 4578 admissions with any antibiotic prescription, but from the first day of antibiotic treatment for only 1602 (58·9%) of 2721 admissions in Geneva. For those for whom the CDSS was not used from the first day, mean time to use of CDSS was 8·9 days. Based on the manual review of 1195 randomly selected charts, transition from intravenous to oral therapy was significantly more frequent in the intervention group after adjusting for confounders (154 [76·6%] of 201 vs 187 [87%] of 215, +10·4%; OR 1·9, 95% CI 1·1-3·3). Consultations by infectious disease specialists were less frequent in the intervention group (388 [13·4%] of 2889) versus the control group (405 [16·9%] of 2390; OR 0·84, 95% CI 0·59-1·25).
An integrated multimodal computerised antibiotic stewardship intervention did not significantly reduce overall antibiotic use, the primary outcome of the study. Contributing factors were probably insufficient uptake, a setting with relatively low antibiotic use at baseline, and delays between ward admission and first CDSS use.
Swiss National Science Foundation.
For the French and Italian translations of the abstract see Supplementary Materials section.
计算机化决策支持系统(CDSS)可辅助医生合理开具抗生素,从而有助于实现抗生素管理。然而,有关其对抗生素使用数量和质量影响的高质量证据仍然稀缺。我们的研究旨在评估一种结合抗生素使用指标反馈的计算机化决策支持系统是否能减少成年住院患者的抗生素处方量。
计算机化抗生素管理研究(COMPASS)是一项多中心、集群随机、平行组、开放性优效性试验,旨在评估一种多模式计算机化抗生素管理干预是否能有效减少成年住院患者的抗生素使用。经过配对匹配后,瑞士三家三级和二级保健医院的 24 个病房(1:1)被随机分配到 CDSS 干预组或使用在线随机序列发生器的标准抗生素管理措施组。多模式干预包括提供选择、持续时间和重新评估抗菌治疗支持的 CDSS,以及抗生素使用质量反馈。主要结局是每例患者入院的总体全身抗生素使用天数,使用调整后的门槛负二项混合效应模型进行分析。分析按照意向治疗和方案进行。该研究在 ClinicalTrials.gov 上注册(标识符 NCT03120975)。
2018 年 10 月 1 日至 2019 年 12 月 31 日,24 个集群(日内瓦大学医院 16 个,提契诺州立医院 8 个)符合条件并随机分组到对照组或干预组。共有 4578 例(11384 例患者的 40.2%)在干预组和 4142 例(9673 例患者的 42.8%)在对照组中接受了抗生素治疗。干预组每例患者入院的平均抗生素使用天数略低于对照组(每例患者入院的治疗天数 3.2 天,SD 6.2,vs 每例患者入院的治疗天数 3.5 天,SD 6.8;p<0.0001),且接受抗生素治疗的患者之间的治疗天数相似(每例患者入院的治疗天数 7.9 天,SD 7.6,vs 每例患者入院的治疗天数 8.1 天,SD 8.4;p=0.50)。调整混杂因素后,两组接受抗生素治疗的入院患者的抗生素使用比例差异无统计学意义(干预组与对照组的比值比为 1.12,95%CI 0.94-1.33)。对于有抗生素暴露的住院患者,每日治疗天数也相似(发病率比 0.98,95%CI 0.90-1.07)。总体而言,在接受任何抗生素处方的 4578 例入院患者中,CDSS 的使用至少为 1 次,在日内瓦的 2721 例入院患者中,只有 1602 例(58.9%)从抗生素治疗的第一天就开始使用 CDSS。对于那些从第一天开始就没有使用 CDSS 的患者,使用 CDSS 的平均时间为 8.9 天。根据 1195 份随机选择的图表的手动审查,在调整混杂因素后,干预组从静脉到口服治疗的转换明显更频繁(201 例中的 154 例[76.6%],215 例中的 187 例[87.0%],+10.4%;OR 1.9,95%CI 1.1-3.3)。感染病专家的会诊在干预组(2889 例中的 388 例[13.4%])比对照组(2390 例中的 405 例[16.9%])少(OR 0.84,95%CI 0.59-1.25)。
一种集成的多模式计算机化抗生素管理干预措施并没有显著减少总体抗生素使用,这是研究的主要结局。可能的促成因素是吸收不足、基线抗生素使用相对较低的环境以及病房入院和首次 CDSS 使用之间的延迟。
瑞士国家科学基金会。