Division of Anesthesia and Intensive Care, Department of Clinical Sciences Lund, Helsingborg Hospital, Lund University, Svartbrödragränden 3, 251 87, Helsingborg, Sweden.
Department of Critical Care, Maine Medical Center, Portland, ME, USA.
Neurocrit Care. 2023 Feb;38(1):16-25. doi: 10.1007/s12028-022-01564-6. Epub 2022 Jul 28.
Sedation and analgesia are recommended during targeted temperature management (TTM) after cardiac arrest, but there are few data to provide guidance on dosing to bedside clinicians. We evaluated differences in patient-level sedation and analgesia dosing in an international multicenter TTM trial to better characterize current practice and clinically important outcomes.
A total 950 patients in the international TTM trial were randomly assigned to a TTM of 33 °C or 36 °C after resuscitation from cardiac arrest in 36 intensive care units. We recorded cumulative doses of sedative and analgesic drugs at 12, 24, and 48 h and normalized to midazolam and fentanyl equivalents. We compared number of medications used, dosing, and titration among centers by using multivariable models, including common severity of illness factors. We also compared dosing with time to awakening, incidence of clinical seizures, and survival.
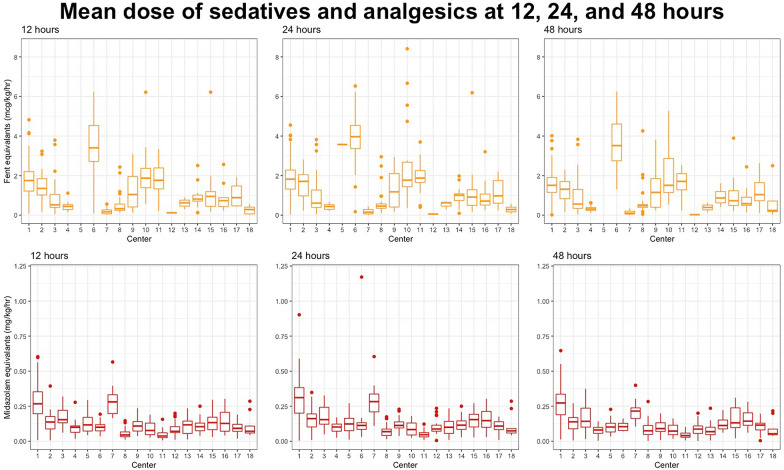
A total of 614 patients at 18 centers were analyzed. Propofol (70%) and fentanyl (51%) were most frequently used. The average dosages of midazolam and fentanyl equivalents were 0.13 (0.07, 0.22) mg/kg/h and 1.16 (0.49, 1.81) µg/kg/h, respectively. There were significant differences in number of medications (p < 0.001), average dosages (p < 0.001), and titration at all time points between centers (p < 0.001), and the outcomes of patients in these centers were associated with all parameters described in the multivariate analysis, except for a difference in the titration of sedatives between 12 and 24 h (p = 0.40). There were associations between higher dosing at 48 h (p = 0.003, odds ratio [OR] 1.75) and increased titration of analgesics between 24 and 48 h (p = 0.005, OR 4.89) with awakening after 5 days, increased titration of sedatives between 24 and 48 h with awakening after 5 days (p < 0.001, OR > 100), and increased titration of sedatives between 24 and 48 h with a higher incidence of clinical seizures in the multivariate analysis (p = 0.04, OR 240). There were also significant associations between decreased titration of analgesics and survival at 6 months in the multivariate analysis (p = 0.048).
There is significant variation in choice of drug, dosing, and titration when providing sedation and analgesics between centers. Sedation and analgesia dosing and titration were associated with delayed awakening, incidence of clinical seizures, and survival, but the causal relation of these findings cannot be proven.
心脏骤停后建议进行目标温度管理(TTM)时进行镇静和镇痛,但目前很少有数据可以为临床医生提供剂量指导。我们评估了一项国际多中心 TTM 试验中患者镇静和镇痛剂量的差异,以便更好地描述当前的实践和临床重要结局。
950 例患者随机分配至复苏后 33°C 或 36°C 的 TTM 治疗,来自 36 个重症监护病房。我们记录了 12、24 和 48 小时时镇静和镇痛药物的累积剂量,并以咪达唑仑和芬太尼当量进行了标准化。我们使用多变量模型比较了中心之间药物使用数量、剂量和滴定,包括常见的严重疾病因素。我们还比较了剂量与唤醒时间、临床癫痫发作发生率和存活率。
共分析了来自 18 个中心的 614 例患者。丙泊酚(70%)和芬太尼(51%)最常使用。咪达唑仑和芬太尼当量的平均剂量分别为 0.13(0.07,0.22)mg/kg/h 和 1.16(0.49,1.81)μg/kg/h。中心之间药物数量(p<0.001)、平均剂量(p<0.001)和滴定均存在显著差异(p<0.001),且这些中心的患者结局与多变量分析中描述的所有参数相关,除了镇静剂 12 至 24 小时的滴定差异(p=0.40)。48 小时时更高的剂量(p=0.003,比值比[OR]1.75)和 24 至 48 小时时镇痛剂的更高滴定(p=0.005,OR 4.89)与 5 天后的觉醒有关,24 至 48 小时时镇静剂的更高滴定与 5 天后的觉醒有关(p<0.001,OR>100),24 至 48 小时时镇静剂的更高滴定与多变量分析中的临床癫痫发作发生率较高有关(p=0.04,OR 240)。在多变量分析中,24 至 48 小时时镇痛剂的剂量降低与 6 个月时的存活率有关(p=0.048)。
在镇静和镇痛方面,不同中心之间药物选择、剂量和滴定存在显著差异。镇静和镇痛的剂量和滴定与唤醒延迟、临床癫痫发作发生率和存活率有关,但这些发现的因果关系无法证明。