Division of Cardiology, Severance Hospital Yonsei University College of Medicine Seoul Korea.
Department of Preventive Medicine Yonsei University College of Medicine Seoul Korea.
J Am Heart Assoc. 2022 Aug 2;11(15):e026375. doi: 10.1161/JAHA.121.026375. Epub 2022 Jul 29.
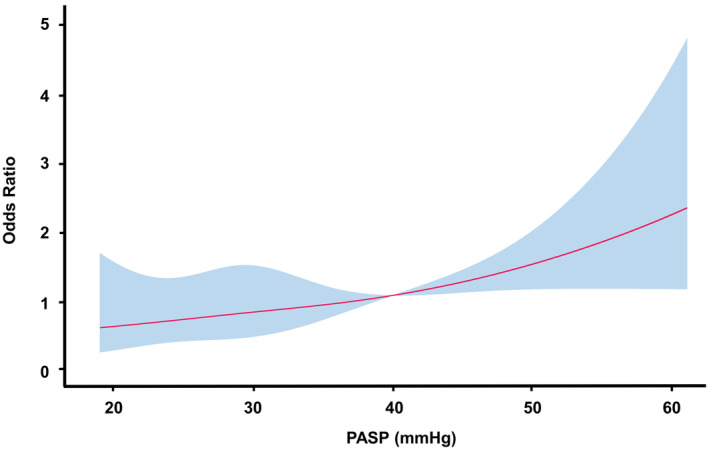
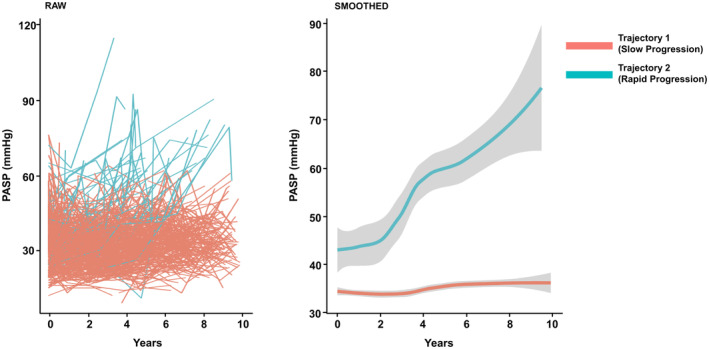
Background Rheumatic mitral stenosis is a significant cause of valvular heart disease. Pulmonary arterial systolic pressure (PASP) reflects the hemodynamic consequences of mitral stenosis and is used to determine treatment strategies. However, PASP progression and expected outcomes based on PASP changes in patients with moderately severe mitral stenosis remain unclear. Methods and Results A total of 436 patients with moderately severe rheumatic mitral stenosis (valve area 1.0-1.5 cm) were enrolled. Composite outcomes included all-cause mortality and hospitalization for heart failure. Data-driven phenotyping identified 2 distinct trajectory groups based on PASP progression: rapid (8.7%) and slow (91.3%). Patients in the rapid progression group were older and had more diabetes and atrial fibrillation than those in the slow progression group (all <0.05). The initial mean diastolic pressure gradient and PASP were higher in the rapid progression group than in the slow progression group (6.2±2.4 mm Hg versus 5.1±2.0 mm Hg [=0.001] and 42.3±13.3 mm Hg versus 33.0±9.2 mm Hg [<0.001], respectively). The rapid progression group had a poorer event-free survival rate than the slow progression group (log-rank <0.001). Rapid PASP progression was a significant risk factor for composite outcomes even after adjusting for comorbidities (hazard ratio, 3.08 [95% CI, 1.68-5.64]; <0.001). Multivariate regression analysis revealed that PASP >40 mm Hg was independently associated with allocation to the rapid progression group (odds ratio, 4.95 [95% CI, 2.08-11.99]; <0.001). Conclusions Rapid PASP progression was associated with a higher risk of the composite outcomes. The main independent predictor for rapid progression group allocation was initial PASP >40 mm Hg.
背景
风湿性二尖瓣狭窄是瓣膜性心脏病的一个重要病因。肺动脉收缩压(PASP)反映了二尖瓣狭窄的血流动力学后果,用于确定治疗策略。然而,中度严重二尖瓣狭窄患者的 PASP 进展和基于 PASP 变化的预期结果尚不清楚。
方法和结果
共纳入 436 例中度严重风湿性二尖瓣狭窄(瓣口面积 1.0-1.5cm)患者。复合结局包括全因死亡率和心力衰竭住院。基于 PASP 进展情况,数据驱动的表型分析确定了 2 个不同的轨迹组:快速(8.7%)和缓慢(91.3%)。快速进展组患者年龄较大,糖尿病和心房颤动的发生率高于缓慢进展组(均<0.05)。快速进展组的初始平均舒张期压力梯度和 PASP 高于缓慢进展组(6.2±2.4mmHg 与 5.1±2.0mmHg [=0.001]和 42.3±13.3mmHg 与 33.0±9.2mmHg [<0.001])。快速进展组无事件生存率低于缓慢进展组(对数秩检验<0.001)。即使在校正合并症后,快速 PASP 进展也是复合结局的显著危险因素(风险比,3.08[95%置信区间,1.68-5.64];<0.001)。多变量回归分析显示,PASP>40mmHg 与被分配到快速进展组独立相关(优势比,4.95[95%置信区间,2.08-11.99];<0.001)。
结论
快速 PASP 进展与复合结局的风险增加相关。快速进展组分配的主要独立预测因素是初始 PASP>40mmHg。