Chen Ting, Xie Ruixiang, Zhao Qiuling, Cai Hongfu, Yang Lin
Department of Pharmacy, Fujian Medical University Cancer Hospital, Fujian Cancer Hospital, Fuzhou, China.
Department of Pharmacy, Fujian Medical University Union Hospital, Fuzhou, China.
Front Oncol. 2022 Jul 22;12:746526. doi: 10.3389/fonc.2022.746526. eCollection 2022.
To evaluate the cost utility of camrelizumab plus standard chemotherapy versus standard chemotherapy alone as a first-line treatment for advanced nonsquamous non-small cell lung cancer (NSCLC) from the perspective of the Chinese health care system and to provide a reference for health decision-making.
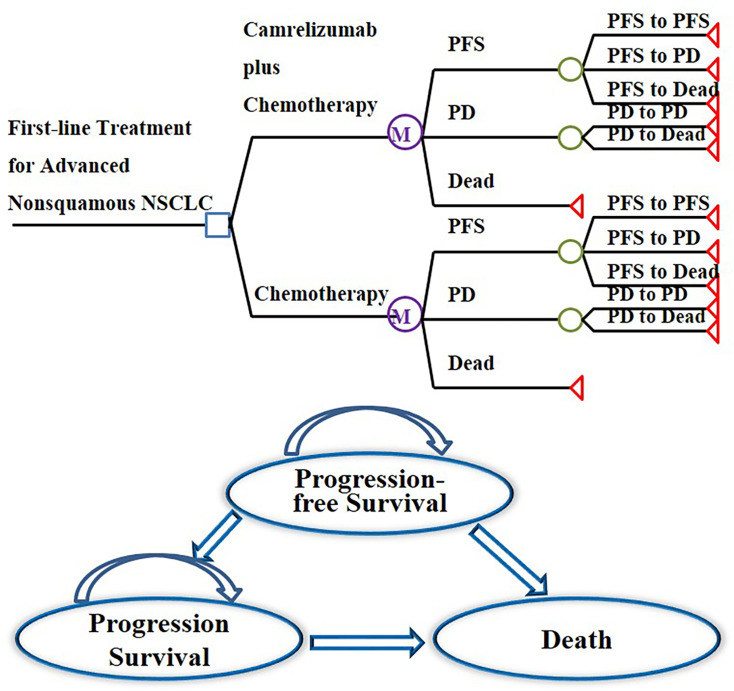
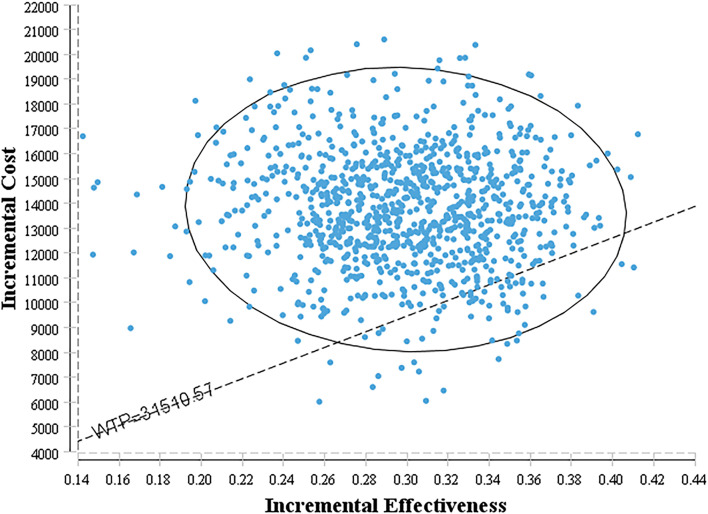
A Markov model consisting of three health states was designed to evaluate the cost utility of these two treatment regimens for NSCLC patients with the incremental cost-effectiveness ratio (ICER) as the primary output indicator. Clinical data were derived from a published phase III clinical trial (CameL; ClinicalTrials.gov; NCT03134872). One-way sensitivity analysis and probabilistic sensitivity analysis were performed to assess the model uncertainty.
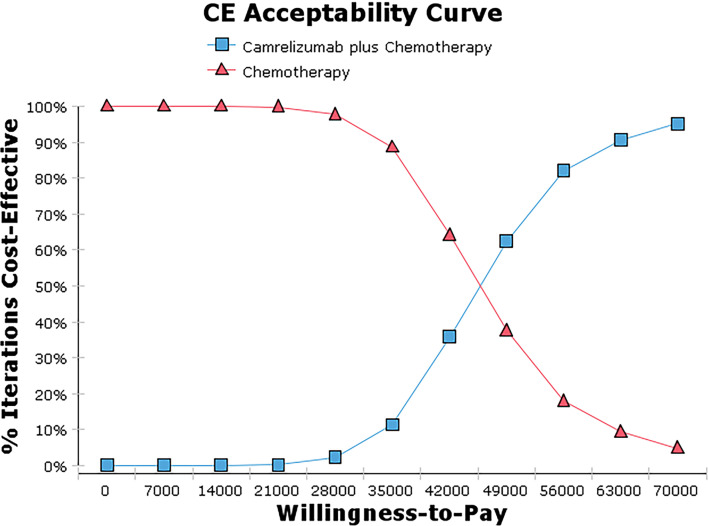
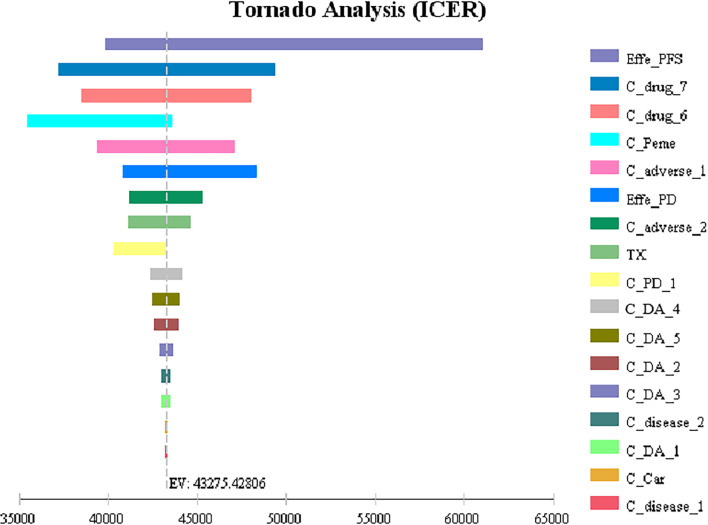
Base case analysis showed that the ICER of camrelizumab plus chemotherapy compared with chemotherapy alone was $43,275.43 per QALY. It was higher than the willingness-to-pay (WTP) threshold of $31,510.57 per QALY in China, which has a standard of three times the GDP per capita recommended by the WHO. One-way sensitivity analysis showed that the utility value of PFS had the greatest influence on the results, and the other sensitive parameters were the cost of subsequent second-line therapy in the two group, the pemetrexed price, the cost of adverse event management and the utility value of PD. The probability sensitivity analysis showed that the probabilities of the cost-effectiveness of camrelizumab plus standard chemotherapy were 27.1%, 66.7% and 88.0% when the WTP values were $40,000, $50,000 and $60,000 per QALY, respectively.
Taking three times the GDP per capita in China as the WTP threshold, the camrelizumab plus standard chemotherapy regimen does not have a cost-effectiveness advantage compared with the standard chemotherapy regimen alone as a first-line treatment for advanced NSCLC.
从中国医疗保健系统的角度评估卡瑞利珠单抗联合标准化疗与单纯标准化疗作为晚期非鳞状非小细胞肺癌(NSCLC)一线治疗的成本效用,为卫生决策提供参考。
设计一个由三种健康状态组成的马尔可夫模型,以增量成本效果比(ICER)作为主要输出指标,评估这两种治疗方案对NSCLC患者的成本效用。临床数据来自一项已发表的III期临床试验(CameL;ClinicalTrials.gov;NCT03134872)。进行单向敏感性分析和概率敏感性分析以评估模型的不确定性。
基础病例分析显示,卡瑞利珠单抗联合化疗与单纯化疗相比,ICER为每质量调整生命年(QALY)43,275.43美元。高于中国每QALY 31,510.57美元的支付意愿(WTP)阈值,该阈值是世界卫生组织推荐的人均国内生产总值的三倍。单向敏感性分析表明,无进展生存期(PFS)的效用值对结果影响最大,其他敏感参数为两组后续二线治疗的成本、培美曲塞价格、不良事件管理成本和疾病进展(PD)的效用值。概率敏感性分析显示,当WTP值分别为每QALY 40,000美元、50,000美元和60,000美元时,卡瑞利珠单抗联合标准化疗具有成本效果的概率分别为27.1%、66.7%和88.0%。
以中国三倍人均国内生产总值作为WTP阈值,卡瑞利珠单抗联合标准化疗方案作为晚期NSCLC一线治疗与单纯标准化疗方案相比不具有成本效果优势。