Division of Infectious Diseases, Department of Medicine, Korea University School of Medicine, Seoul, South Korea.
Division of Infectious Diseases, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, 81 Irwon-ro, Gangnam-gu, Seoul, 06351, South Korea.
BMC Infect Dis. 2022 Aug 10;22(1):686. doi: 10.1186/s12879-022-07668-w.
To find pharmacokinetic/pharmacodynamic parameters of vancomycin associated with the optimal outcome of severe infection due to Enterococcus species.
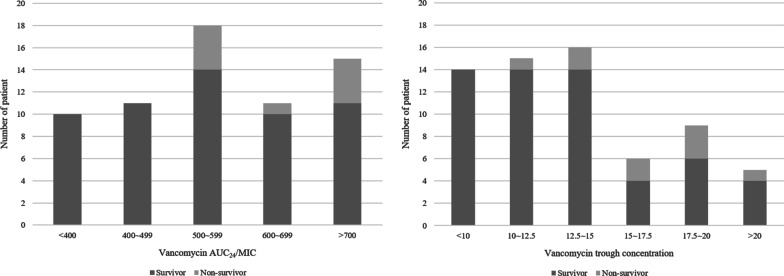
We retrospectively reviewed enterococcal bacteremia cases treated with vancomycin from January 2015 to December 2020. The primary outcome was 30-day mortality. We calculated cutoff values of the ratio of vancomycin area under the concentration-time curve over 24 h to the minimum inhibitory concentration (AUC/MIC) and trough concentration (C) during the initial 72 h of treatment. The optimal cutoff value was determined using the Youden index. Binary variables created based on these cutoffs were further assessed using multivariable analysis.
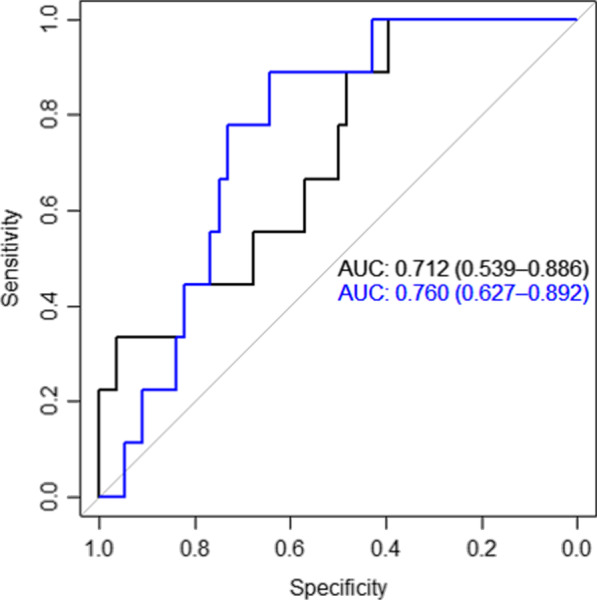
A total of 65 patients were included. The majority (87.7%) had solid or hematologic malignancies. Thirty-day mortality and nephrotoxicity occurred in nine (13.4%) and 14 (21.5%) patients, respectively. Both vancomycin AUC/MIC and C showed fair performance in predicting 30-day mortality (AUC of receiver-operator curve for AUC/MIC, 0.712; 95% confidence interval [CI] 0.539-0.886; AUC for C, 0.760; 95% CI 0.627-0.892; pairwise AUC comparison: p = 0.570). C ≥ 13.94 μg/mL, but not AUC/MIC ≥ 504, had a significant association with 30-day mortality after adjusting for confounders (odds ratio, 8.40; 95% CI 1.60-86.62; p = 0.010).
Mean C ≥ 13.94 μg/mL during the initial 72 h was associated with higher 30-day mortality in enterococcal bacteremia. Further studies are warranted to elucidate optimal pharmacokinetic targets for enterococcal bacteremia.
寻找与肠球菌属严重感染最佳疗效相关的万古霉素药代动力学/药效学参数。
我们回顾性分析了 2015 年 1 月至 2020 年 12 月期间接受万古霉素治疗的肠球菌菌血症病例。主要结局为 30 天死亡率。我们计算了治疗开始后 72 小时内的万古霉素 24 小时浓度-时间曲线下面积与最低抑菌浓度(AUC/MIC)和谷浓度(C)比值的截断值。使用约登指数确定最佳截断值。基于这些截断值创建的二变量进一步使用多变量分析进行评估。
共纳入 65 例患者。大多数(87.7%)患者患有实体或血液系统恶性肿瘤。9 例(13.4%)和 14 例(21.5%)患者分别发生 30 天死亡率和肾毒性。万古霉素 AUC/MIC 和 C 对 30 天死亡率均有较好的预测性能(AUC/MIC 的接受者操作特征曲线 AUC,0.712;95%置信区间 [CI],0.539-0.886;C 的 AUC,0.760;95%CI,0.627-0.892;两两 AUC 比较:p=0.570)。在调整混杂因素后,C≥13.94μg/mL,但 AUC/MIC≥504 与 30 天死亡率无显著相关性(优势比,8.40;95%CI,1.60-86.62;p=0.010)。
肠球菌菌血症治疗开始后 72 小时内的平均 C≥13.94μg/mL 与 30 天死亡率升高相关。需要进一步研究以阐明肠球菌菌血症的最佳药代动力学目标。