Department of Surgery, Amsterdam UMC Location University of Amsterdam, Amsterdam, The Netherlands.
Cancer Treatment and Quality of Life, Cancer Center Amsterdam, Amsterdam, The Netherlands.
Updates Surg. 2023 Feb;75(2):281-290. doi: 10.1007/s13304-022-01347-w. Epub 2022 Aug 13.
Gastrectomy with lymph node dissection is the cornerstone of curative treatment of gastric cancer. Extent of lymphadenectomy may differ depending on T-stage, as the rate of lymph node metastases may differ. The objective of this systematic review is to investigate and compare the prevalence of nodal metastases in the individual lymph node stations between different T-stages.
Data reporting and structure of this systematic review follows the PRISMA checklist. The Medline and PubMed databases were systematically searched. The search included the following Mesh terms: "Stomach Neoplasms", "Lymphatic Metastasis" and "Lymph Node Excision". The primary outcome was the highest prevalence of nodal metastases per T-stage.
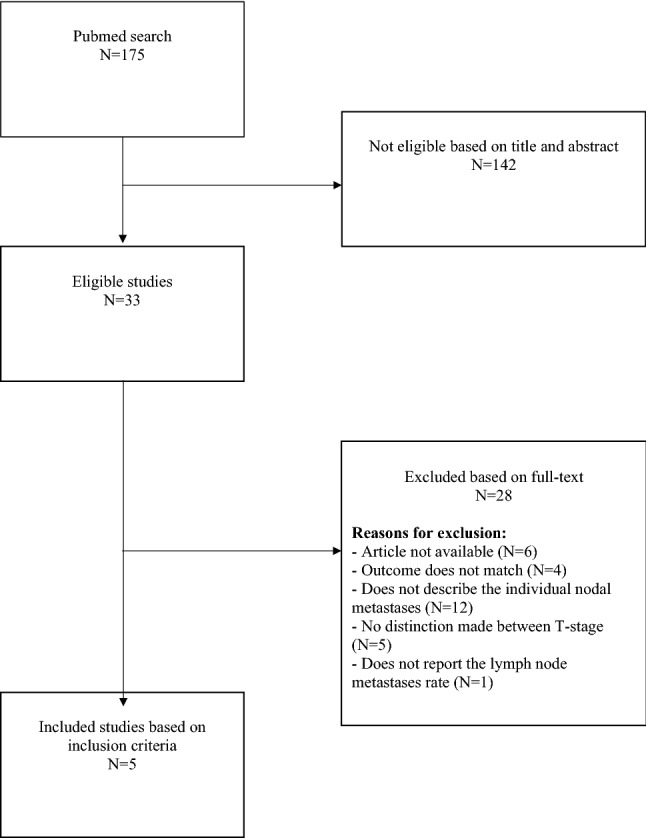
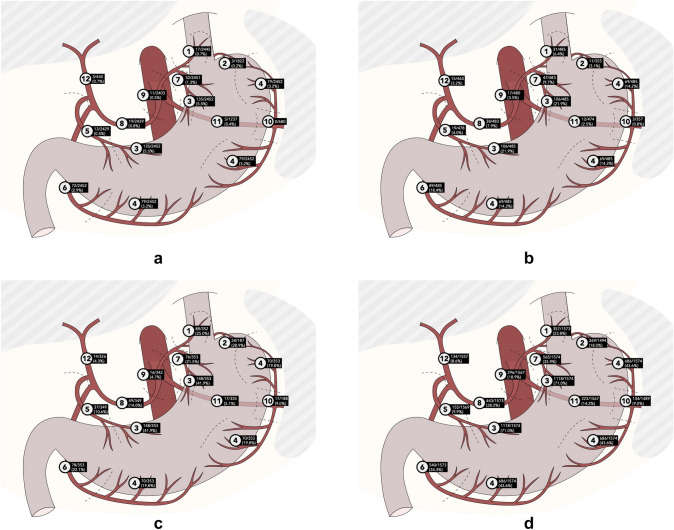
The initial search resulted in 175 eligible articles. Five articles met the inclusion criteria and were accordingly analyzed. Concerning the lymph node stations 1 to 7, the lymph nodes along the lesser gastric curvature (station 3) show the highest metastases rate (T1: 5.5%, T2: 21.9%, T3: 41.9%, T4: 71.0%). Concerning the lymph node stations 8 to 20, the lymph nodes around the common hepatic artery (station 8) show the highest metastases rate (T1: 0.8%, T2: 7.9%, T3: 14.0%, T4: 28.2%).
An overall low prevalence of nodal metastases in the individual lymph node stations in early, T1 gastric carcinomas and an overall high prevalence in more advanced, T3 and T4 gastric carcinomas endorse a more tailored approach based on the different gastric T-stages. In addition, a less extensive lymphadenectomy seems justified in early T1 carcinoma.
This systematic review provides an overview of the prevalence of nodal metastases for the individual lymph node stations between different T-stages, showing an overall low prevalence in early, T1 gastric carcinomas and an overall high prevalence in the more advanced, T3 and T4 gastric carcinomas.
胃切除术和淋巴结清扫术是胃癌治愈治疗的基石。淋巴结清扫的范围可能因 T 分期而异,因为淋巴结转移的发生率可能不同。本系统综述的目的是调查和比较不同 T 分期的各个淋巴结站的淋巴结转移率。
本系统综述的数据报告和结构遵循 PRISMA 清单。系统检索了 Medline 和 PubMed 数据库。搜索包括以下 MeSH 术语:“胃肿瘤”、“淋巴转移”和“淋巴结切除术”。主要结局是每个 T 分期的淋巴结转移率最高。
最初的搜索结果产生了 175 篇符合条件的文章。符合纳入标准的文章有 5 篇,因此进行了分析。关于淋巴结站 1 至 7,沿小胃曲率的淋巴结(站 3)显示出最高的转移率(T1:5.5%,T2:21.9%,T3:41.9%,T4:71.0%)。关于淋巴结站 8 至 20,肝总动脉周围的淋巴结(站 8)显示出最高的转移率(T1:0.8%,T2:7.9%,T3:14.0%,T4:28.2%)。
早期 T1 胃癌的各个淋巴结站的淋巴结转移率总体较低,晚期 T3 和 T4 胃癌的淋巴结转移率总体较高,支持基于不同的胃 T 分期采取更有针对性的方法。此外,在早期 T1 癌中,淋巴结清扫范围较小似乎是合理的。
本系统综述提供了不同 T 分期的各个淋巴结站的淋巴结转移率的概述,显示早期 T1 胃癌的淋巴结转移率总体较低,晚期 T3 和 T4 胃癌的淋巴结转移率总体较高。