Zheng Guanhao, Cai Jiaqi, Zhang Liang, Chen Dayu, Wang Linyu, Qiu Yusi, Deng Han, Bai Hao, Bian Xiaolan, He Juan
Department of Pharmacy, Ruijin Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai, China.
Department of Pharmacy, Shanghai Chest Hospital, Shanghai Jiao Tong University, Shanghai, China.
Infect Dis Ther. 2022 Oct;11(5):1917-1934. doi: 10.1007/s40121-022-00682-0. Epub 2022 Aug 17.
Considering the importance of ceftazidime/avibactam (CAZ/AVI) and polymyxin B (PMB) in treating carbapenem-resistant Klebsiella pneumoniae (CRKP) infection, it is essential to evaluate the efficacy and safety of these agents and provide appropriate medical advice to clinical specialists.
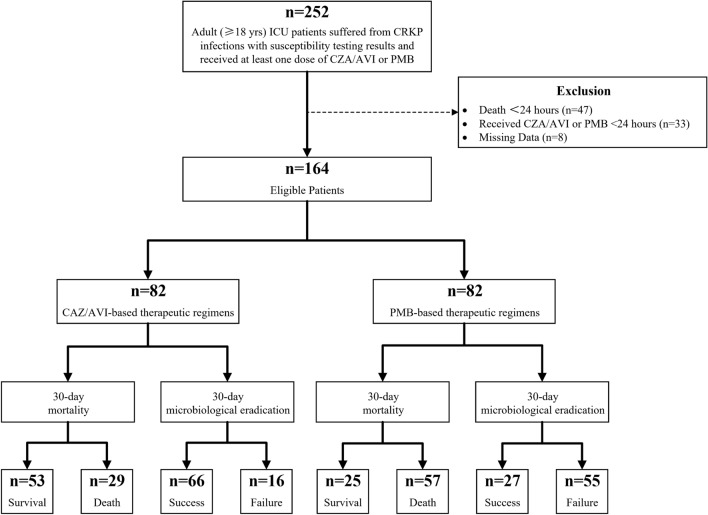
We conducted a retrospective cohort study in two Chinese tertiary hospitals for critically ill patients with CRKP infection who received at least 24-h CAZ/AVI-based or PMB-based treatment. A binary logistic model and a Cox proportional hazards regression model were constructed to analyze variables that could potentially affect 30-day microbiological eradication and all-cause mortality, respectively.
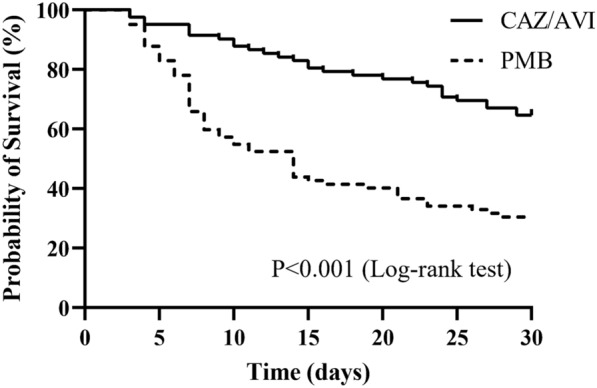
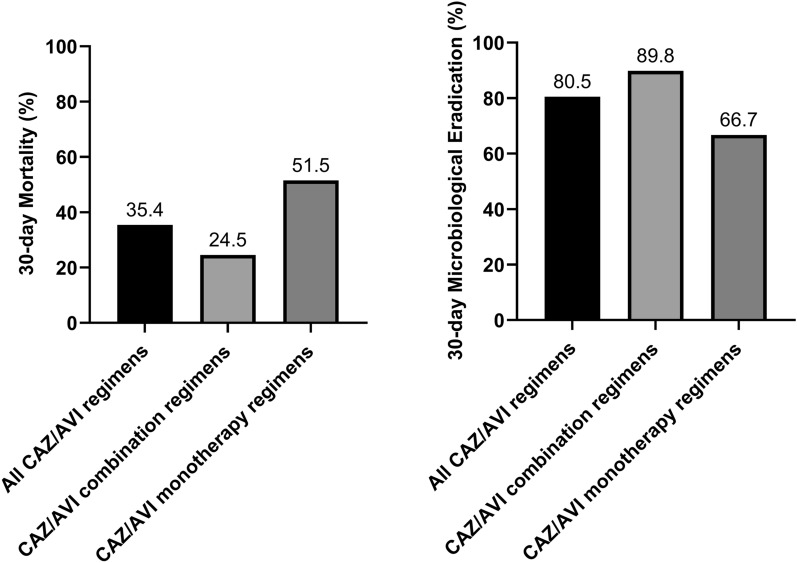
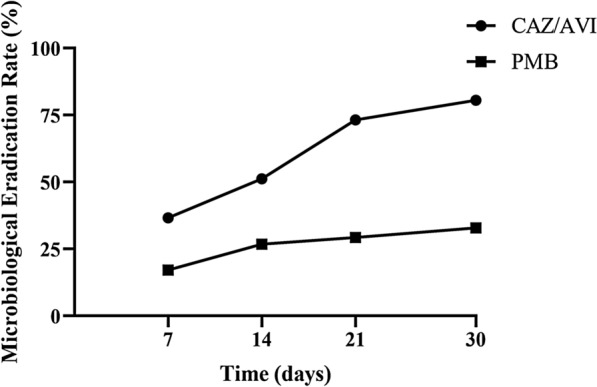
From January 2019 to December 2021, 164 eligible patients were divided into CAZ/AVI and PMB cohorts. A notably lower 30-day mortality rate (35.4% vs 69.5%, P < 0.001) and a higher 30-day microbiological eradication rate (80.5% vs 32.9%, P < 0.001) were observed for patients receiving CAZ/AVI-based treatment, compared with cases in the PMB group. A longer antimicrobial treatment duration (> 7 days) could also significantly decrease the mortality rate and increase the microbiological eradication rate. Female patients had a higher survival rate than male patients. Age over 65 years, sepsis, continuous renal replacement therapy, and organ transplantation were identified as negative factors for survival. In the subgroup analysis, CAZ/AVI combined with tigecycline or amikacin could effectively lower mortality. According to safety evaluation results, potential elevation of hepatic enzymes was associated with CAZ/AVI-based treatment, while renal impairment was probably related to PMB-based treatment.
CAZ/AVI was more effective than PMB in treating CRKP-infected patients. Tigecycline and amikacin were proven to be beneficial as concomitant agents in combination with CAZ/AVI. A treatment period lasting over 7 days was recommended. Hepatoxicity of CAZ/AVI and nephrotoxicity of PMB should be monitored carefully. Further well-designed studies should be performed to verify our conclusion.
鉴于头孢他啶/阿维巴坦(CAZ/AVI)和多粘菌素B(PMB)在治疗耐碳青霉烯类肺炎克雷伯菌(CRKP)感染中的重要性,评估这些药物的疗效和安全性并为临床专科医生提供适当的医学建议至关重要。
我们在两家中国三级医院对接受至少24小时基于CAZ/AVI或基于PMB治疗的CRKP感染重症患者进行了一项回顾性队列研究。构建二元逻辑模型和Cox比例风险回归模型,分别分析可能影响30天微生物清除率和全因死亡率的变量。
2019年1月至2021年12月,164例符合条件的患者被分为CAZ/AVI组和PMB组。与PMB组患者相比,接受基于CAZ/AVI治疗的患者30天死亡率显著更低(35.4%对69.5%,P<0.001),30天微生物清除率更高(80.5%对32.9%,P<0.001)。更长的抗菌治疗持续时间(>7天)也可显著降低死亡率并提高微生物清除率。女性患者的生存率高于男性患者。65岁以上、脓毒症、持续肾脏替代治疗和器官移植被确定为生存的负面因素。在亚组分析中,CAZ/AVI联合替加环素或阿米卡星可有效降低死亡率。根据安全性评估结果,基于CAZ/AVI的治疗与肝酶潜在升高有关,而肾功能损害可能与基于PMB的治疗有关。
CAZ/AVI在治疗CRKP感染患者方面比PMB更有效。已证明替加环素和阿米卡星作为与CAZ/AVI联合使用的伴随药物有益。建议治疗期持续超过7天。应仔细监测CAZ/AVI的肝毒性和PMB的肾毒性。应进行进一步精心设计的研究以验证我们的结论。