Hamad Medical Corporation, Doha, Qatar.
Department of Radiology, Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts, United States of America.
PLoS One. 2022 Aug 19;17(8):e0273227. doi: 10.1371/journal.pone.0273227. eCollection 2022.
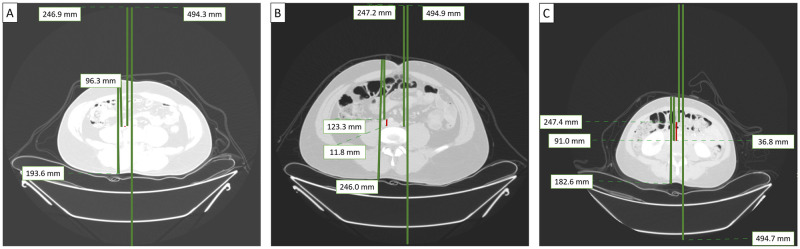
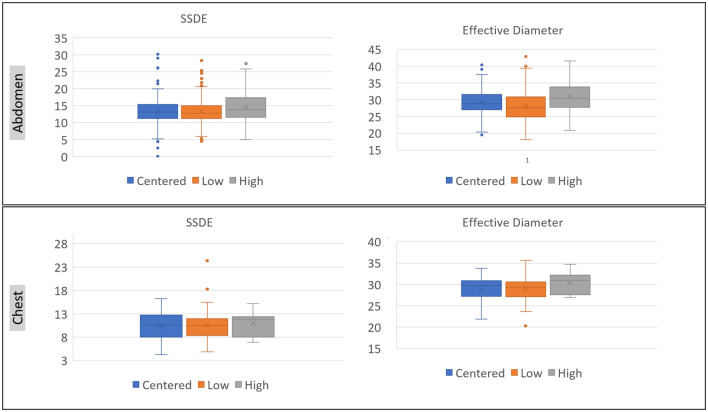
There are no published data on the effect of patient and technologist gender and ethnicity attributes on off-centering in CT. Therefore, we assessed the impact of patient and technologist variations on off-centering patients undergoing body CT. With institutional review board approval, our retrospective study included 1000 consecutive adult patients (age ranged 22-96 years; 756 males: 244 females) who underwent chest or abdomen CT examinations. We recorded patient (age, gender, nationality, body weight, height,), technologist gender, and scan-related (scanner vendor, body region imaged, scan length, CT dose index volume, dose length product) information. Lateral and anteroposterior (AP) diameters were recorded to calculate effective diameter and size-specific dose estimate (SSDE). Off-centering represented the distance between the anterior-posterior centers of the scan field of view and the patient at the level of carina (for chest CT) and iliac crest (for abdomen CT). About 76% of the patients (760/1000) were off-centered with greater off-centering for chest (22 mm) than for abdomen (15 mm). Although ethnicity or patient gender was not a significant determinant of off-centering, technologist-patient gender mismatch was associated with a significantly greater frequency of off-centering (p<0.001). Off-centering below the gantry isocenter was twice as common as off-centering above the gantry isocenter (p<0.001). The latter occurred more frequently in larger patients and was associated with higher radiation doses than those centered below the isocenter (p<0.001). Technologists' years of experience and patient factors profoundly affect the presence and extent of off-centering for both chest and abdomen CTs. Larger patients are more often off-centered than smaller patients.
目前尚无关于患者和技师的性别和种族特征对 CT 中心偏移的影响的相关数据。因此,我们评估了患者和技师的变化对行体部 CT 检查的患者中心偏移的影响。本回顾性研究经机构审查委员会批准,纳入了 1000 例连续成年患者(年龄 22-96 岁;男 756 例,女 244 例),这些患者行胸部或腹部 CT 检查。我们记录了患者(年龄、性别、国籍、体重、身高)、技师性别以及与扫描相关的信息(扫描仪供应商、成像的身体部位、扫描长度、CT 剂量指数体积、剂量长度乘积)。记录了侧位和前后位(AP)直径,以计算有效直径和大小特异性剂量估计值(SSDE)。中心偏移代表扫描野中心与隆突(胸部 CT)和髂嵴(腹部 CT)水平患者中心之间的距离。大约 76%的患者(760/1000)存在中心偏移,胸部的中心偏移(22mm)比腹部的更大(15mm)。尽管种族或患者性别不是中心偏移的重要决定因素,但技师-患者性别不匹配与中心偏移的频率显著增加有关(p<0.001)。与扫描架等中心上方的中心偏移相比,扫描架等中心下方的中心偏移更为常见(p<0.001)。后者在较大的患者中更为常见,且与位于等中心下方的患者相比,其辐射剂量更高(p<0.001)。技师的工作年限和患者因素深刻地影响了胸部和腹部 CT 的中心偏移的存在和程度。较大的患者比较小的患者更容易出现中心偏移。