Department of Orthopaedics, Leiden University Medical Center, Leiden, the Netherlands.
Department of Neurosurgery, Leiden University Medical Center, Leiden, the Netherlands.
Clin Orthop Relat Res. 2022 Dec 1;480(12):2392-2405. doi: 10.1097/CORR.0000000000002311. Epub 2022 Aug 24.
Traumatic brachial plexus injuries (BPIs) in the nerve roots of C5 to T1 lead to the devastating loss of motor and sensory function in the upper extremity. Free functional gracilis muscle transfer (FFMT) is used to reconstruct elbow and shoulder function in adults with traumatic complete BPIs. The question is whether the gains in ROM and functionality for the patient outweigh the risks of such a large intervention to justify this surgery in these patients.
QUESTIONS/PURPOSES: (1) After FFMT for adult traumatic complete BPI, what is the functional recovery in terms of elbow flexion, shoulder abduction, and wrist extension (ROM and muscle grade)? (2) Does the choice of distal insertion affect the functional recovery of the elbow, shoulder, and wrist? (3) Does the choice of nerve source affect elbow flexion and shoulder abduction recovery? (4) What factors are associated with less residual disability? (5) What proportion of flaps have necrosis and do not reinnervate?
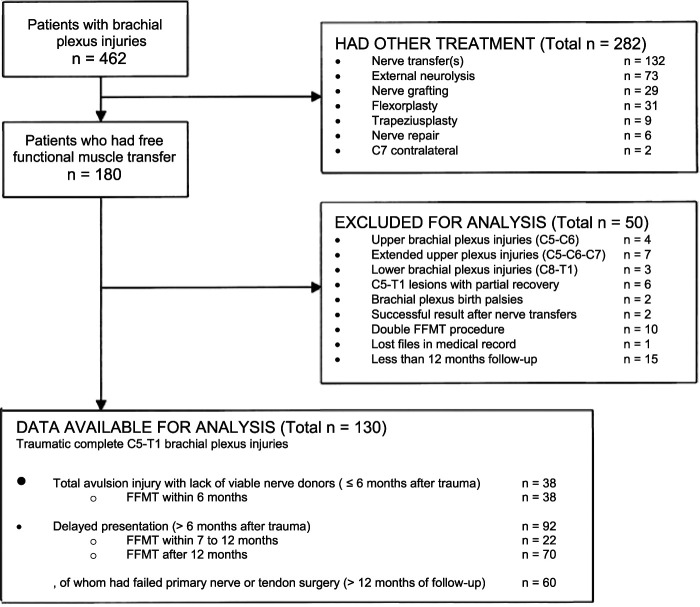
We performed a retrospective observational study at Dr. Soetomo General Hospital in Surabaya, Indonesia. A total of 180 patients with traumatic BPIs were treated with FFMT between 2010 and 2020, performed by a senior orthopaedic hand surgeon with 14 years of experience in FFMT. We included patients with traumatic complete C5 to T1 BPIs who underwent a gracilis FFMT procedure. Indications were total avulsion injuries and delayed presentation (>6 months after trauma) or after failed primary nerve transfers (>12 months). Patients with less than 12 months of follow-up were excluded, leaving 130 patients eligible for this study. The median postoperative follow-up period was 47 months (interquartile range [IQR] 33 to 66 months). Most were men (86%; 112 of 130) who had motorcycle collisions (96%; 125 patients) and a median age of 23 years (IQR 19 to 34 years). Orthopaedic surgeons and residents measured joint function at the elbow (flexion), shoulder (abduction), and wrist (extension) in terms of British Medical Research Council (MRC) muscle strength scores and active ROM. A univariate analysis of variance test was used to evaluate these outcomes in terms of differences in distal attachment to the extensor carpi radialis brevis (ECRB), extensor digitorum communis and extensor pollicis longus (EDC/EPL), the flexor digitorum profundus and flexor pollicis longus (FDP/FPL), and the choice of a phrenic, accessory, or intercostal nerve source. We measured postoperative function with the DASH score and pain at rest with the VAS score. A multivariate linear regression analysis was performed to investigate what patient and injury factors were associated with less disability. Complications such as flap necrosis, innervation problems, infections, and reoperations were evaluated.
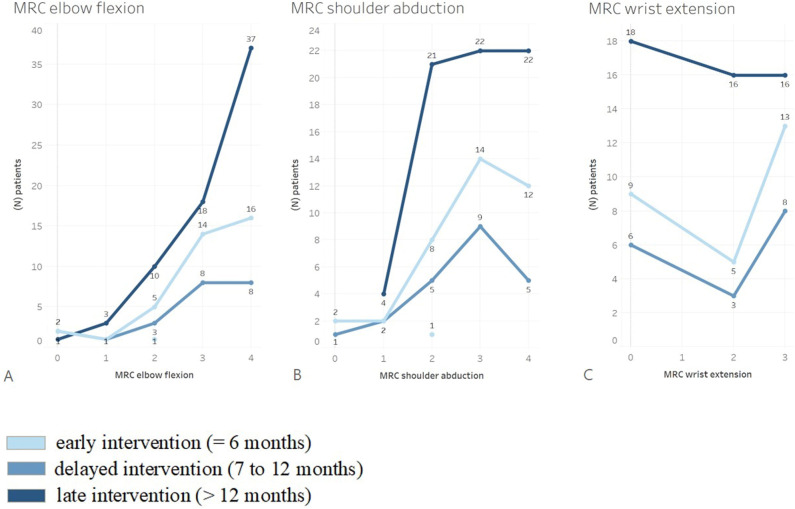
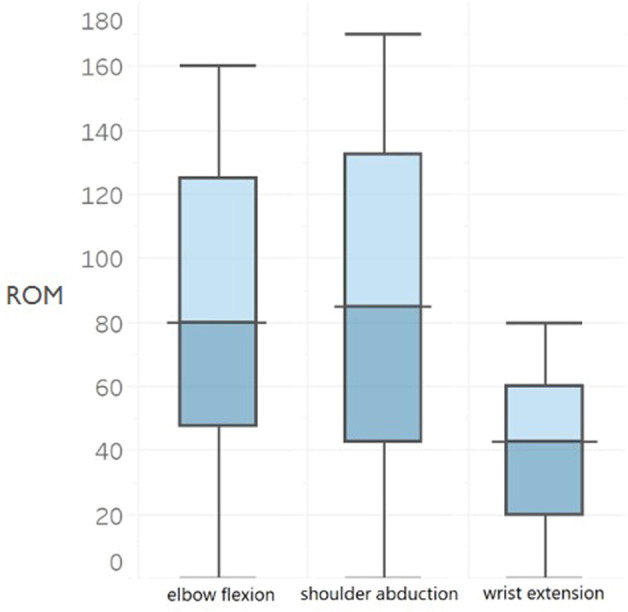
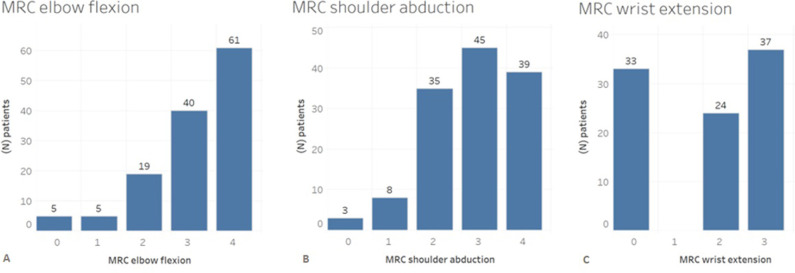
The median elbow flexion muscle strength was 3 (IQR 3 to 4) and active ROM was 88° ± 46°. The median shoulder abduction grade was 3 (IQR 2 to 4) and active ROM was 62° ± 42°. However, the choice of distal insertion was not associated with differences in the median wrist extension strength (ECRB: 2 [IQR 0 to 3], EDC/EPL: 2 [IQR 0 to 3], FDP/FPL: 1 [IQR 0 to 2]; p = 0.44) or in ROM (ECRB: 21° ± 19°, EDC/EPL: 21° ± 14°, FDP/FPL: 13° ± 15°; p = 0.69). Furthermore, the choice of nerve source did not affect the mean ROM for elbow flexion (phrenic nerve: 87° ± 46°; accessory nerve: 106° ± 49°; intercostal nerves: 103° ± 50°; p = 0.55). No associations were found with less disability (lower DASH scores): young age (coefficient = 0.28; 95% CI -0.22 to 0.79; p = 0.27), being a woman (coefficient = -9.4; 95% CI -24 to 5.3; p = 0.20), and more postoperative months (coefficient = 0.02; 95% CI -0.01 to 0.05]; p = 0.13). The mean postoperative VAS score for pain at rest was 3 ± 2. Flap necrosis occurred in 5% (seven of 130) of all patients, and failed innervation of the gracilis muscle occurred in 4% (five patients).
FFMT achieves ROM with fair-to-good muscle power of elbow flexion, shoulder abduction, and overall function for the patient, but does not achieve good wrist function. Meticulous microsurgical skills and extensive rehabilitation training are needed to maximize the result of FFMT. Further technical developments in distal attachment and additional nerve procedures will pave the way for reconstructing a functional limb in patients with a flail upper extremity.
Level III, therapeutic study.
C5 到 T1 神经根的创伤性臂丛神经损伤导致上肢运动和感觉功能严重丧失。游离功能性股薄肌转移(FFMT)用于重建成人创伤性完全臂丛神经损伤的肘部和肩部功能。问题是,对于这些患者,这种大干预的 ROM 和功能增益是否超过了风险,从而证明这种手术是合理的。
问题/目的:(1)成人创伤性完全 BPI 行 FFMT 后,肘部屈曲、肩部外展和腕关节伸展的功能恢复情况如何(ROM 和肌肉等级)?(2)远端附着点的选择是否会影响肘部、肩部和腕部的功能恢复?(3)神经源的选择是否会影响屈肘和肩外展的恢复?(4)哪些因素与残余残疾程度较低相关?(5)有多少比例的皮瓣坏死且无法重新支配?
我们在印度尼西亚泗水的苏腊巴亚(Soetomo)综合医院进行了一项回顾性观察性研究。2010 年至 2020 年期间,共有 180 例创伤性臂丛神经损伤患者接受了 FFMT,由一位具有 14 年 FFMT 经验的资深骨科手外科医生进行。我们纳入了创伤性 C5 到 T1 完全臂丛神经损伤且接受股薄肌 FFMT 手术的患者。适应证为完全撕脱伤和延迟出现(创伤后>6 个月)或初次神经转移失败(>12 个月)。排除了随访时间少于 12 个月的患者,共 130 例患者符合本研究条件。中位术后随访时间为 47 个月(四分位距[IQR]33 至 66 个月)。大多数患者为男性(86%;112/130),均因摩托车事故受伤(96%;125 例),中位年龄为 23 岁(IQR 19 至 34 岁)。矫形外科医生和住院医师根据英国医学研究委员会(MRC)肌肉力量评分和主动 ROM 评估肘部(屈曲)、肩部(外展)和腕部(伸展)的关节功能。使用单因素方差分析检验来评估远端附着于桡侧腕短伸肌(ECRB)、指总伸肌和拇长伸肌(EDC/EPL)、指深屈肌和拇长屈肌(FDP/FPL)以及膈神经、副神经或肋间神经源选择的差异。我们使用 DASH 评分测量术后功能,使用 VAS 评分测量休息时的疼痛。进行多元线性回归分析,以探讨哪些患者和损伤因素与残疾程度较低相关。评估并发症,如皮瓣坏死、神经支配问题、感染和再手术。
中位肘部屈曲肌肉力量为 3(IQR 3 至 4),主动 ROM 为 88°±46°。中位肩部外展肌力为 3(IQR 2 至 4),主动 ROM 为 62°±42°。然而,远端插入点的选择与中位腕关节伸展力量(ECRB:2[IQR 0 至 3]、EDC/EPL:2[IQR 0 至 3]、FDP/FPL:1[IQR 0 至 2])或 ROM(ECRB:21°±19°、EDC/EPL:21°±14°、FDP/FPL:13°±15°)均无差异(p=0.44)。此外,神经源的选择也不影响屈肘的平均 ROM(膈神经:87°±46°;副神经:106°±49°;肋间神经:103°±50°;p=0.55)。与较低的残疾程度(较低的 DASH 评分)无关联:年轻(系数=0.28;95%CI-0.22 至 0.79;p=0.27)、女性(系数=-9.4;95%CI-24 至 5.3;p=0.20)、术后时间更长(系数=0.02;95%CI-0.01 至 0.05;p=0.13)。中位术后休息时 VAS 评分疼痛为 3±2。所有患者中有 5%(7/130)出现皮瓣坏死,4%(5 例)出现股薄肌神经支配失败。
FFMT 实现了 ROM,肘部屈曲、肩部外展和整体功能的肌肉力量为患者提供了良好到尚可的效果,但腕关节功能不佳。需要精细的显微外科技能和广泛的康复训练,以最大限度地提高 FFMT 的效果。远端附着点和附加神经手术的进一步技术发展将为上肢瘫痪患者重建功能性肢体铺平道路。
III 级,治疗性研究。