Division of Hematology, School of Medicine, University of Colorado, Aurora, Colorado.
Abramson Cancer Center, University of Pennsylvania, Philadelphia, Pennsylvania.
Clin Cancer Res. 2022 Dec 15;28(24):5272-5279. doi: 10.1158/1078-0432.CCR-22-1183.
To evaluate efficacy and safety of venetoclax + azacitidine in treatment-naïve patients with acute myeloid leukemia harboring poor-risk cytogenetics and TP53mut or TP53wt.
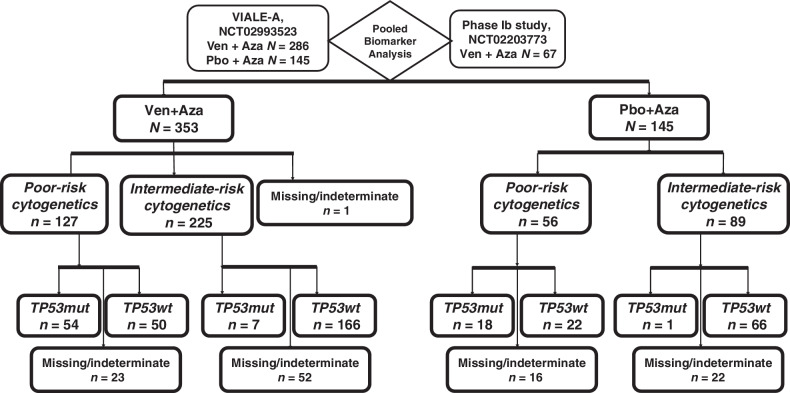
We analyzed data from a phase III study (NCT02993523) comparing venetoclax (400 mg orally days 1-28) + azacitidine (75 mg/m2 days 1-7) or placebo + azacitidine, and from a phase Ib study (NCT02203773) of venetoclax + azacitidine. Patients were ineligible for intensive therapy. TP53 status was analyzed centrally; cytogenetic studies were performed locally.
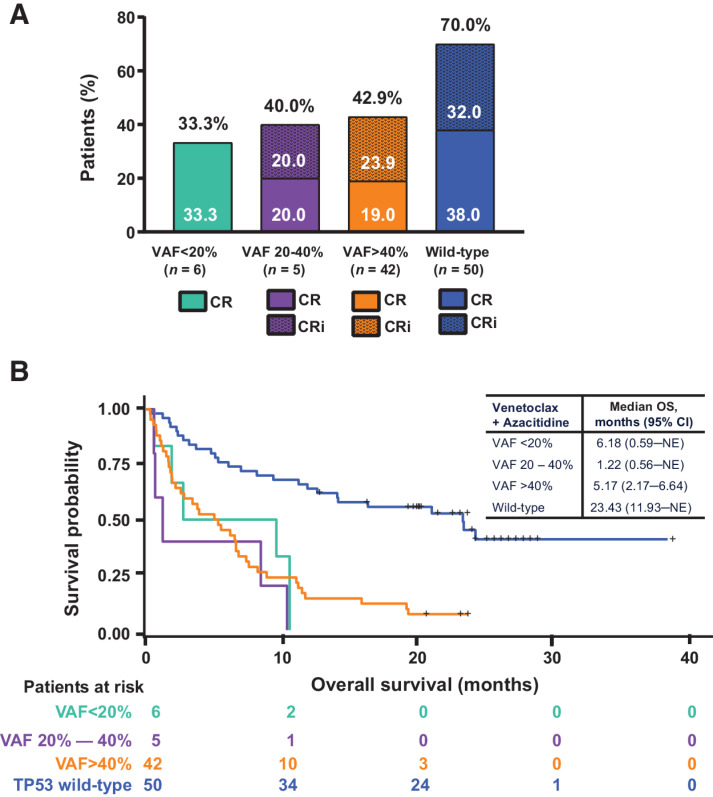
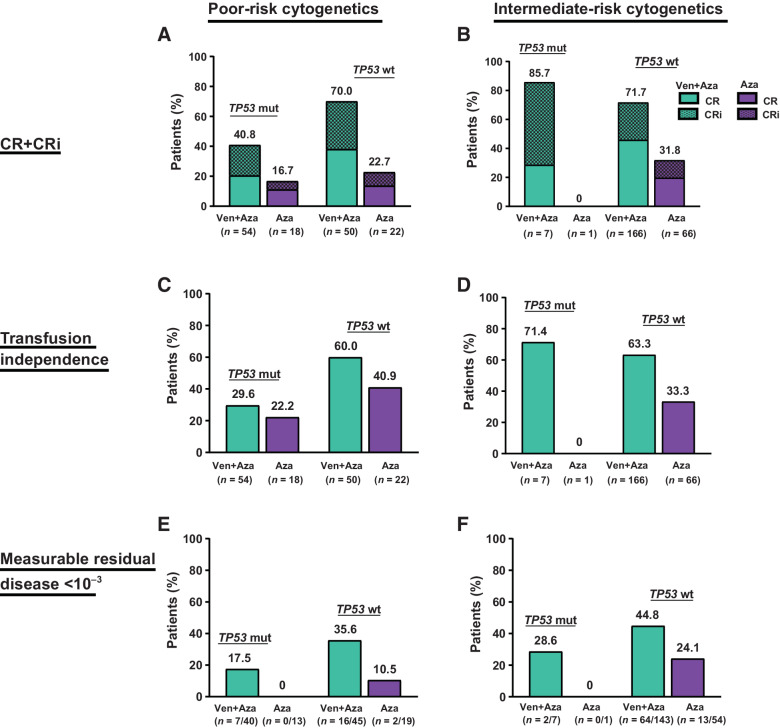
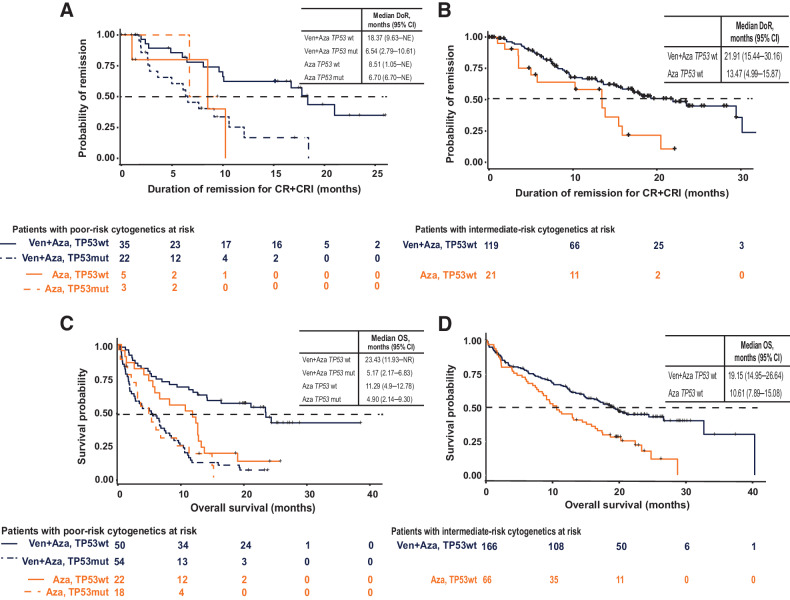
Patients (n = 127) with poor-risk cytogenetics receiving venetoclax + azacitidine (TP53wt = 50; TP53mut = 54) were compared with patients with poor-risk cytogenetics (n = 56) receiving azacitidine alone (TP53wt = 22; TP53mut = 18).For poor-risk cytogenetics + TP53wt patients, venetoclax + azacitidine versus azacitidine alone resulted in composite remission rates (CRc) of 70% versus 23%, median duration of remission (DoR) of 18.4 versus 8.5 months, and median overall survival (OS) of 23.4 versus 11.3 months, respectively. Outcomes with venetoclax + azacitidine were comparable with similarly treated patients with intermediate-risk cytogenetics and TP53wt.For poor-risk cytogenetics + TP53mut patients, venetoclax + azacitidine versus azacitidine alone resulted in CRc of 41% versus 17%, median DoR of 6.5 versus 6.7 months, and median OS of 5.2 versus 4.9 months, respectively.For poor-risk cytogenetics + TP53mut patients, predominant grade ≥3 adverse events (AE) for venetoclax + azacitidine versus azacitidine were febrile neutropenia (55%/39%), thrombocytopenia (28%/28%), neutropenia (26%/17%), anemia (13%/6%), and pneumonia (28%/33%). AEs were comparable between TP53mut and TP53wt patients.
In poor-risk cytogenetics + TP53mut patients, venetoclax + azacitidine improved remission rates but not DoR or OS compared with azacitidine alone. However, in poor-risk cytogenetics + TP53wt patients, venetoclax + azacitidine resulted in higher remission rates and longer DoR and OS than azacitidine alone, with outcomes comparable with similarly treated patients with intermediate-risk cytogenetics. Toxicities were similar in TP53mut and TP53wt patients. See related commentary by Green and Zeidner, p. 5235.
评估 venetoclax + 阿扎胞苷治疗初治伴不良细胞遗传学和 TP53 突变或 TP53wt 的急性髓系白血病患者的疗效和安全性。
我们分析了一项比较 venetoclax(400 mg 口服,第 1-28 天)+ 阿扎胞苷(75 mg/m2,第 1-7 天)或安慰剂+阿扎胞苷的 III 期研究(NCT02993523)和 venetoclax + 阿扎胞苷的 Ib 期研究(NCT02203773)的数据。患者不符合强化治疗条件。TP53 状态由中心分析;细胞遗传学研究由当地进行。
接受 venetoclax + 阿扎胞苷治疗的不良细胞遗传学患者(TP53wt = 50;TP53mut = 54)与接受阿扎胞苷单药治疗的不良细胞遗传学患者(TP53wt = 22;TP53mut = 18)进行比较。对于不良细胞遗传学+TP53wt 患者,venetoclax + 阿扎胞苷与阿扎胞苷单药治疗的复合缓解率(CRc)分别为 70%与 23%,缓解持续时间(DoR)中位数分别为 18.4 个月与 8.5 个月,总生存期(OS)中位数分别为 23.4 个月与 11.3 个月。venetoclax + 阿扎胞苷的治疗结果与具有中等风险细胞遗传学和 TP53wt 的相似患者相似。对于不良细胞遗传学+TP53mut 患者,venetoclax + 阿扎胞苷与阿扎胞苷单药治疗的 CRc 分别为 41%与 17%,DoR 中位数分别为 6.5 个月与 6.7 个月,OS 中位数分别为 5.2 个月与 4.9 个月。对于不良细胞遗传学+TP53mut 患者,venetoclax + 阿扎胞苷与阿扎胞苷单药治疗的主要不良事件(AE)发生率≥3 级分别为发热性中性粒细胞减少症(55%/39%)、血小板减少症(28%/28%)、中性粒细胞减少症(26%/17%)、贫血(13%/6%)和肺炎(28%/33%)。TP53mut 和 TP53wt 患者的 AE 相似。
在不良细胞遗传学+TP53mut 患者中,venetoclax + 阿扎胞苷与阿扎胞苷单药治疗相比,缓解率提高,但无进展生存期(DoR)或总生存期(OS)无改善。然而,在不良细胞遗传学+TP53wt 患者中,venetoclax + 阿扎胞苷治疗与阿扎胞苷单药治疗相比,缓解率更高,无进展生存期和总生存期更长,且与具有中等风险细胞遗传学的相似患者的治疗结果相当。TP53mut 和 TP53wt 患者的毒性相似。详见 Green 和 Zeidner 的相关评论,第 5235 页。