Digital Health Research and Innovation, Institute for Clinical Research, National Institutes of Health, Shah Alam, Malaysia; College of Medicine and Veterinary Medicine, University of Edinburgh, Edinburgh, UK.
Anaesthesiology and Intensive Care, Sarawak General Hospital, Kuching, Malaysia.
Lancet Digit Health. 2022 Sep;4(9):e676-e691. doi: 10.1016/S2589-7500(22)00124-8.
Telemedicine has been increasingly integrated into chronic disease management through remote patient monitoring and consultation, particularly during the COVID-19 pandemic. We did a systematic review and meta-analysis of studies reporting effectiveness of telemedicine interventions for the management of patients with cardiovascular conditions.
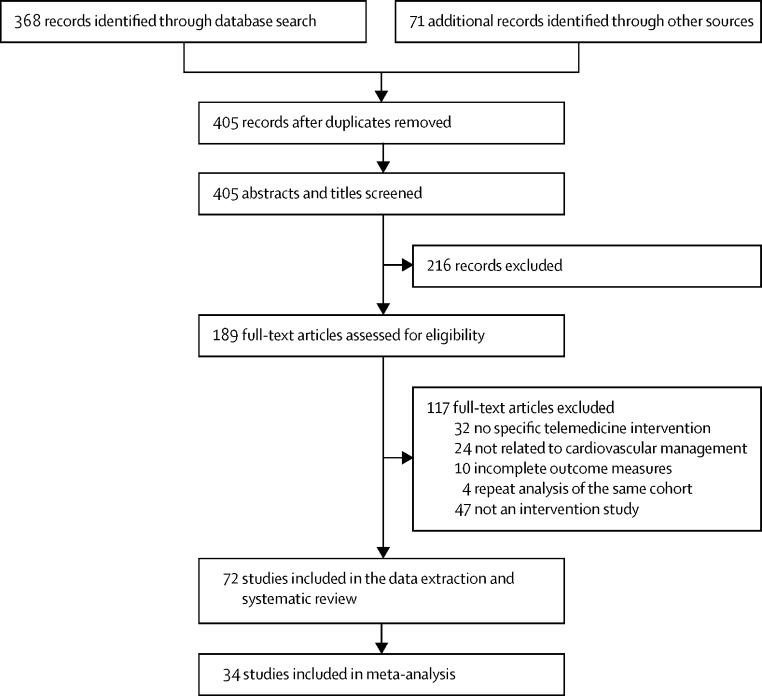
In this systematic review and meta-analysis, we searched PubMed, Scopus, and Cochrane Library from database inception to Jan 18, 2021. We included randomised controlled trials and observational or cohort studies that evaluated the effects of a telemedicine intervention on cardiovascular outcomes for people either at risk (primary prevention) of cardiovascular disease or with established (secondary prevention) cardiovascular disease, and, for the meta-analysis, we included studies that evaluated the effects of a telemedicine intervention on cardiovascular outcomes and risk factors. We excluded studies if there was no clear telemedicine intervention described or if cardiovascular or risk factor outcomes were not clearly reported in relation to the intervention. Two reviewers independently assessed and extracted data from trials and observational and cohort studies using a standardised template. Our primary outcome was cardiovascular-related mortality. We evaluated study quality using Cochrane risk-of-bias and Newcastle-Ottawa scales. The systematic review and the meta-analysis protocol was registered with PROSPERO (CRD42021221010) and the Malaysian National Medical Research Register (NMRR-20-2471-57236).
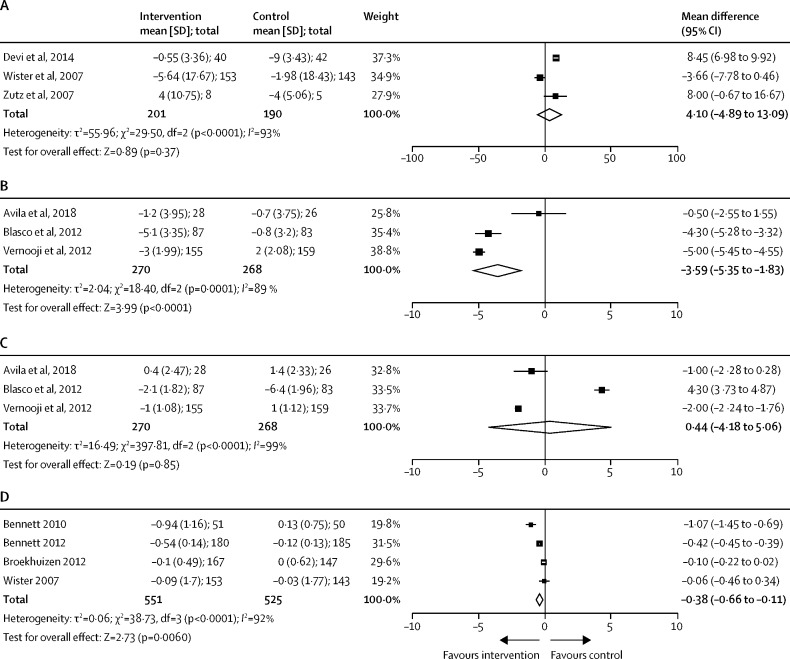
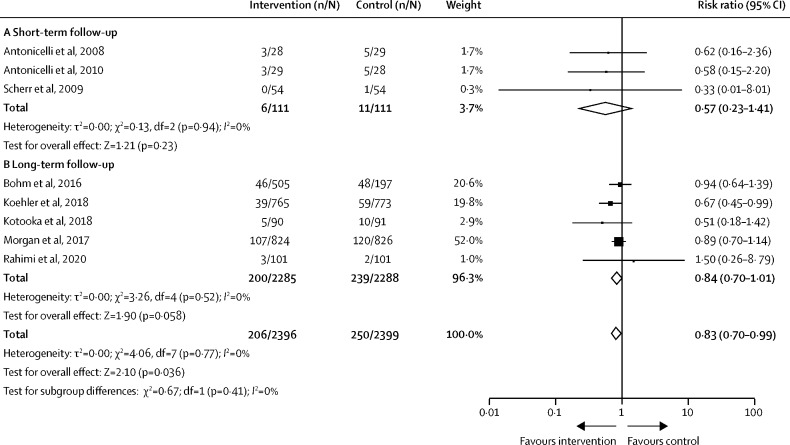
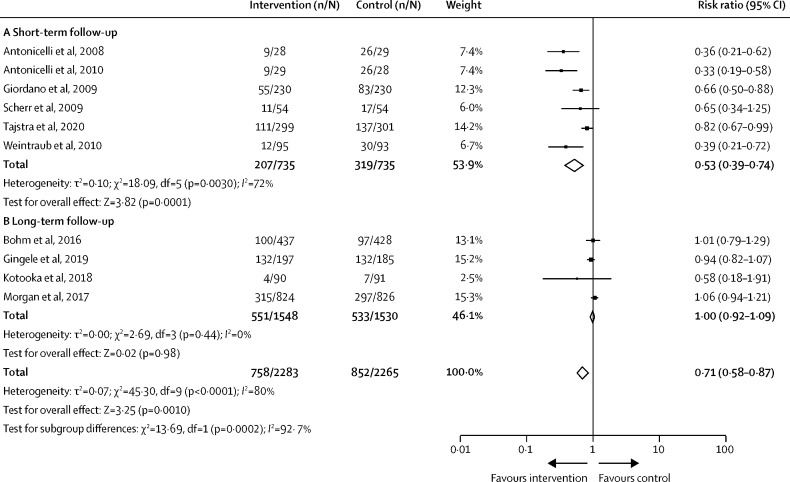
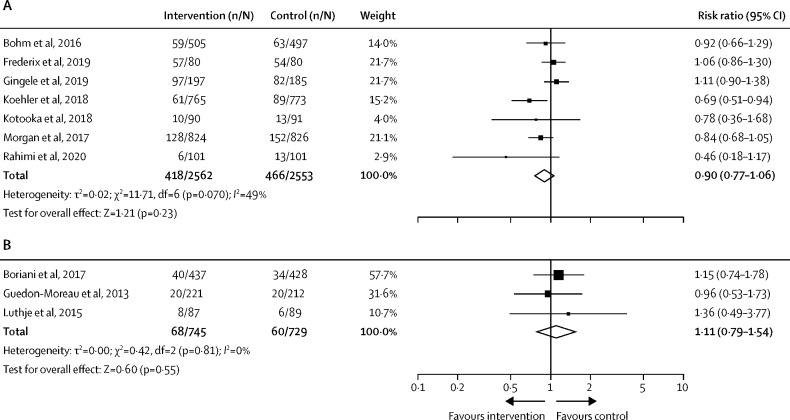
72 studies, including 127 869 participants, met eligibility criteria, with 34 studies included in meta-analysis (n=13 269 with 6620 [50%] receiving telemedicine). Combined remote monitoring and consultation for patients with heart failure was associated with a reduced risk of cardiovascular-related mortality (risk ratio [RR] 0·83 [95% CI 0·70 to 0·99]; p=0·036) and hospitalisation for a cardiovascular cause (0·71 [0·58 to 0·87]; p=0·0002), mostly in studies with short-term follow-up. There was no effect of telemedicine on all-cause hospitalisation (1·02 [0·94 to 1·10]; p=0·71) or mortality (0·90 [0·77 to 1·06]; p=0·23) in these groups, and no benefits were observed with remote consultation in isolation. Small reductions were observed for systolic blood pressure (mean difference -3·59 [95% CI -5·35 to -1·83] mm Hg; p<0·0001) by remote monitoring and consultation in secondary prevention populations. Small reductions were also observed in body-mass index (mean difference -0·38 [-0·66 to -0·11] kg/m; p=0·0064) by remote consultation in primary prevention settings.
Telemedicine including both remote disease monitoring and consultation might reduce short-term cardiovascular-related hospitalisation and mortality risk among patients with heart failure. Future research should evaluate the sustained effects of telemedicine interventions.
The British Heart Foundation.
远程患者监测和咨询使远程医疗越来越多地融入慢性病管理,尤其是在 COVID-19 大流行期间。我们对报告远程医疗干预对心血管疾病患者管理效果的研究进行了系统评价和荟萃分析。
在这项系统评价和荟萃分析中,我们从数据库建立到 2021 年 1 月 18 日在 PubMed、Scopus 和 Cochrane 图书馆进行了搜索。我们纳入了随机对照试验和观察性或队列研究,评估了远程医疗干预对处于心血管疾病风险(一级预防)或已确诊(二级预防)的患者的心血管结局的影响,对于荟萃分析,我们纳入了评估远程医疗干预对心血管结局和风险因素影响的研究。如果没有明确描述远程医疗干预,或者心血管或风险因素结局与干预没有明确报告,我们将排除这些研究。两位审查员使用标准化模板独立评估和提取试验、观察性和队列研究的数据。我们的主要结局是心血管相关死亡率。我们使用 Cochrane 偏倚风险和纽卡斯尔-渥太华量表评估研究质量。系统评价和荟萃分析方案在 PROSPERO(CRD42021221010)和马来西亚国家医学研究登记处(NMRR-20-2471-57236)上进行了注册。
72 项研究,包括 127869 名参与者,符合入选标准,其中 34 项研究纳入荟萃分析(n=13269 人,其中 6620 人[50%]接受远程医疗)。心力衰竭患者的远程监测和咨询联合使用与心血管相关死亡率降低相关(风险比 [RR] 0.83 [95%CI 0.70 至 0.99];p=0.036)和因心血管原因住院(0.71 [0.58 至 0.87];p=0.0002),这主要发生在短期随访的研究中。远程医疗对这些人群的全因住院(1.02 [0.94 至 1.10];p=0.71)或死亡率(0.90 [0.77 至 1.06];p=0.23)没有影响,单独进行远程咨询也没有益处。在二级预防人群中,远程监测和咨询可使收缩压降低 3.59mmHg(95%CI -5.35 至 -1.83];p<0.0001)。在一级预防环境中,远程咨询还可使体重指数降低 0.38kg/m²(平均差值 -0.38 [-0.66 至 -0.11];p=0.0064)。
远程医疗包括远程疾病监测和咨询,可能会降低心力衰竭患者的短期心血管相关住院和死亡风险。未来的研究应评估远程医疗干预的持续效果。
英国心脏基金会。