Department of Medicine, Imperial College London, Faculty of Medicine, London, UK.
Department of Cardiothoracic Surgery, Imperial College NHS Trust, Hammersmith Hospital, London, UK.
J Card Surg. 2022 Nov;37(11):3743-3753. doi: 10.1111/jocs.16890. Epub 2022 Aug 30.
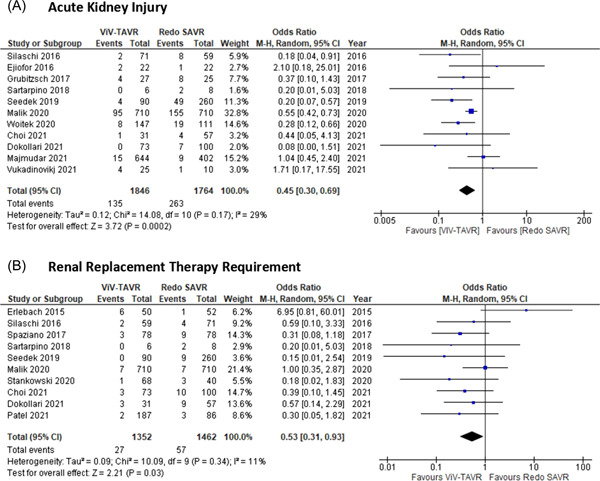
Postoperative acute kidney injury (AKI) and the requirement for renal replacement therapy (RRT) remain common and significant complications of both transcatheter valve-in-valve aortic valve replacement (ViV-TAVR) and redo surgical aortic valve replacement (SAVR). Nevertheless, the understanding of renal outcomes in the population undergoing either redo SAVR or ViV-TAVR remains controversial.
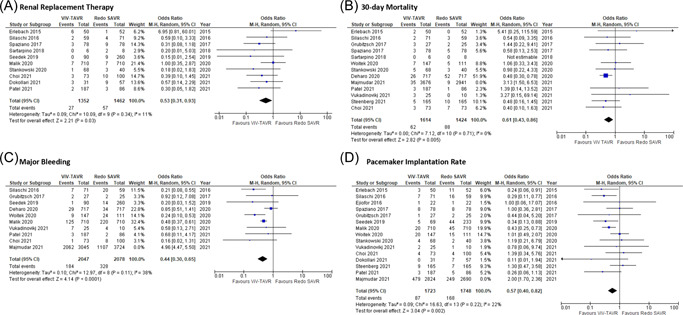
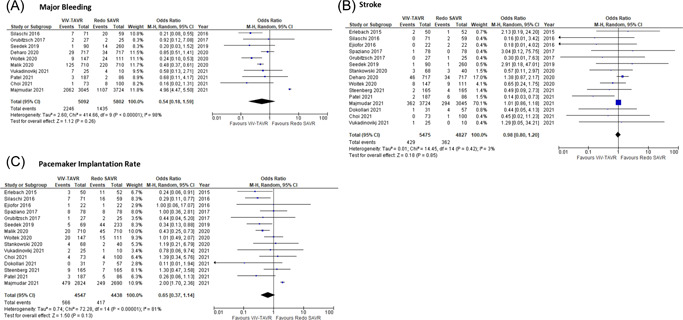
A systematic database search with meta-analysis was conducted of comparative original articles of ViV-TAVR versus redo SAVR in EMBASE, MEDLINE, Cochrane database, and Google Scholar, from inception to September 2021. Primary outcomes were AKI and RRT. Secondary outcomes were stroke, major bleeding, pacemaker implantation rate, operative mortality, and 30-day mortality.
Our search yielded 5435 relevant studies. Eighteen studies met the inclusion criteria with a total of 11,198 patients. We found ViV-TAVR to be associated with lower rates of AKI, postoperative RRT, major bleeding, pacemaker implantation, operative mortality, and 30-day mortality. No significant difference was observed in terms of stroke rate. The mean incidence of AKI in ViV-TAVR was 6.95% (±6%) and in redo SAVR was 15.2% (±9.6%). For RRT, our data showed that VIV-TAVR to be 1.48% (±1.46%) and redo SAVR to be 8.54% (±8.06%).
Renoprotective strategies should be put into place to prevent and reduce AKI incidence regardless of the treatment modality. Patients undergoing re-intervention for the aortic valve constitute a high-risk and frail population in which ViV-TAVR demonstrated it might be a feasible option for carefully selected patients. Long-term follow-up data and randomized control trials will be needed to evaluate mortality and morbidity outcomes between these 2 treatments.
经导管主动脉瓣置换术中瓣中瓣(ViV-TAVR)和再次主动脉瓣置换术(redo SAVR)术后急性肾损伤(AKI)和肾脏替代治疗(RRT)的需求仍然是常见且严重的并发症。然而,对于接受 redo SAVR 或 ViV-TAVR 的患者的肾脏结局的理解仍存在争议。
对 EMBASE、MEDLINE、Cochrane 数据库和 Google Scholar 进行了系统的数据库检索,并进行了荟萃分析,检索时间从建库至 2021 年 9 月。主要结局是 AKI 和 RRT。次要结局是卒中、大出血、起搏器植入率、手术死亡率和 30 天死亡率。
我们的检索结果产生了 5435 项相关研究。18 项研究符合纳入标准,共纳入 11198 例患者。我们发现 ViV-TAVR 与较低的 AKI 发生率、术后 RRT、大出血、起搏器植入、手术死亡率和 30 天死亡率相关。卒中发生率无显著差异。ViV-TAVR 中 AKI 的平均发生率为 6.95%(±6%),redo SAVR 中为 15.2%(±9.6%)。对于 RRT,我们的数据显示,ViV-TAVR 为 1.48%(±1.46%),redo SAVR 为 8.54%(±8.06%)。
无论治疗方式如何,都应采取肾保护策略来预防和降低 AKI 的发生率。对于主动脉瓣再次介入的患者,他们构成了一个高危和脆弱的人群,在这些患者中,ViV-TAVR 可能是一种可行的选择。需要长期随访数据和随机对照试验来评估这两种治疗方法之间的死亡率和发病率结局。