Program in Women's Oncology, Women & Infants Hospital, Providence, RI.
The Royal Marsden NHS Foundation Trust and Institute of Cancer Research, London, United Kingdom.
J Clin Oncol. 2023 Jan 20;41(3):609-617. doi: 10.1200/JCO.22.01549. Epub 2022 Sep 9.
In SOLO1/GOG 3004 (ClinicalTrials.gov identifier: NCT01844986), maintenance therapy with the poly(ADP-ribose) polymerase inhibitor olaparib provided a sustained progression-free survival benefit in patients with newly diagnosed advanced ovarian cancer and a and/or (BRCA) mutation. We report overall survival (OS) after a 7-year follow-up, a clinically relevant time point and the longest follow-up for any poly(ADP-ribose) polymerase inhibitor in the first-line setting.
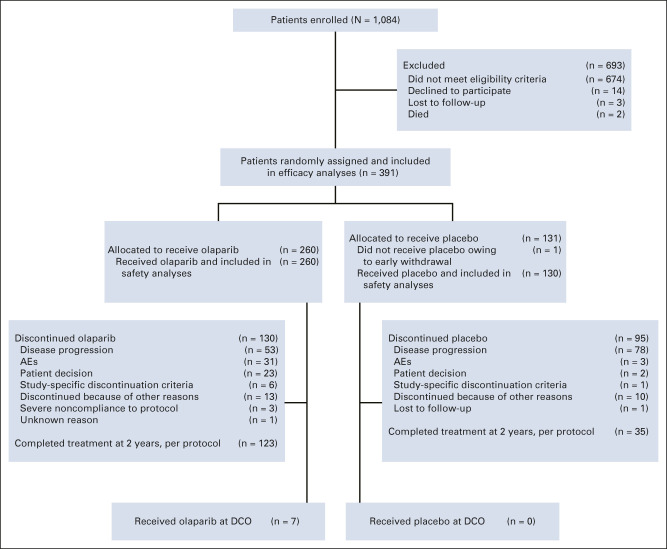
This double-blind phase III trial randomly assigned patients with newly diagnosed advanced ovarian cancer and a BRCA mutation in clinical response to platinum-based chemotherapy to maintenance olaparib (n = 260) or placebo (n = 131) for up to 2 years. A prespecified descriptive analysis of OS, a secondary end point, was conducted after a 7-year follow-up.
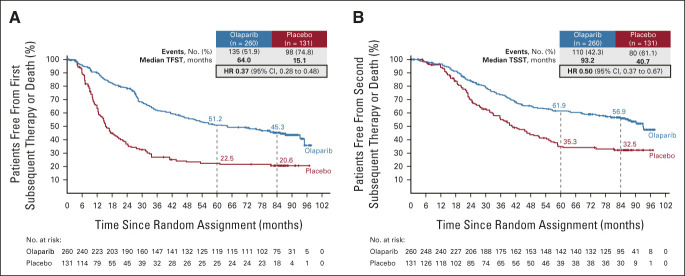
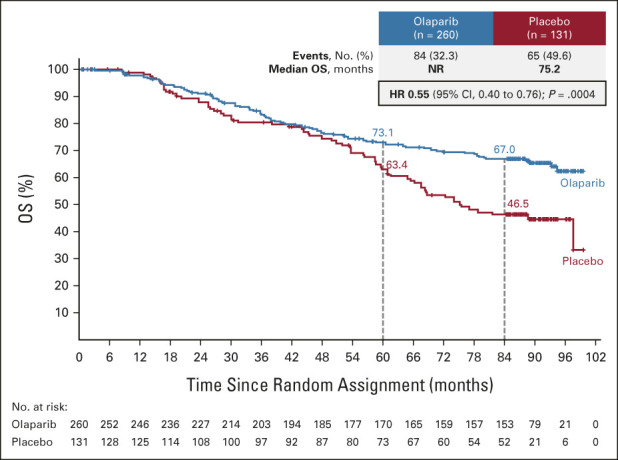
The median duration of treatment was 24.6 months with olaparib and 13.9 months with placebo, and the median follow-up was 88.9 and 87.4 months, respectively. The hazard ratio for OS was 0.55 (95% CI, 0.40 to 0.76; = .0004 [ < .0001 required to declare statistical significance]). At 7 years, 67.0% of olaparib patients versus 46.5% of placebo patients were alive, and 45.3% versus 20.6%, respectively, were alive and had not received a first subsequent treatment (Kaplan-Meier estimates). The incidence of myelodysplastic syndrome and acute myeloid leukemia remained low, and new primary malignancies remained balanced between treatment groups.
Results indicate a clinically meaningful, albeit not statistically significant according to prespecified criteria, improvement in OS with maintenance olaparib in patients with newly diagnosed advanced ovarian cancer and a BRCA mutation and support the use of maintenance olaparib to achieve long-term remission in this setting; the potential for cure may also be enhanced. No new safety signals were observed during long-term follow-up.
在 SOLO1/GOG 3004 研究(ClinicalTrials.gov 标识符:NCT01844986)中,聚(ADP-核糖)聚合酶抑制剂奥拉帕利维持治疗为新诊断的晚期卵巢癌和/或 BRCA 突变患者提供了持续的无进展生存期获益。我们报告了 7 年随访后的总生存期(OS),这是一个具有临床意义的时间点,也是一线治疗中任何聚(ADP-核糖)聚合酶抑制剂最长的随访时间。
这项双盲 III 期试验将临床对铂类化疗有反应的新诊断的晚期卵巢癌和 BRCA 突变患者随机分配接受奥拉帕利(n = 260)或安慰剂(n = 131)维持治疗,最长可达 2 年。在 7 年随访后进行了 OS 的预设描述性分析,这是次要终点。
奥拉帕利组的中位治疗持续时间为 24.6 个月,安慰剂组为 13.9 个月,中位随访时间分别为 88.9 个月和 87.4 个月。OS 的风险比为 0.55(95%CI,0.40 至 0.76;P =.0004[<.0001 为宣布统计学意义所需的数值])。7 年时,奥拉帕利组有 67.0%的患者存活,安慰剂组有 46.5%的患者存活,分别有 45.3%和 20.6%的患者存活且未接受首次后续治疗(Kaplan-Meier 估计)。骨髓增生异常综合征和急性髓系白血病的发生率仍然较低,新原发恶性肿瘤在治疗组之间保持平衡。
结果表明,对于新诊断的晚期卵巢癌和 BRCA 突变患者,奥拉帕利维持治疗可显著改善 OS,尽管根据预设标准,这并非具有统计学意义,但具有临床意义,支持在该治疗环境中使用奥拉帕利维持治疗以实现长期缓解;也可能增强治愈的潜力。在长期随访期间未观察到新的安全性信号。