Monaghan Karen, Cos Travis
University of the West of Scotland, Paisley, UK.
School of Arts and Sciences, La Salle University, Philadelphia, PA, USA.
Med Access Point Care. 2021 Oct 11;5:23992026211050615. doi: 10.1177/23992026211050615. eCollection 2021 Jan-Dec.
Effective and appropriate provision of mental healthcare has long been a struggle globally, resulting in significant disparity between prevalence of mental illness and access to care. One attempt to address such disparity was the Patient Protection and Affordable Care Act (PPACA), 2010, mandate in the United States to integrate physical and mental healthcare in Federally Qualified Health Centers (FQHCs). The notion of integration is attractive, as it has demonstrated the potential to improve both access to mental healthcare and healthcare outcomes. However, while the PPACA mandate set this requirement for FQHCs, no clear process as to how these centers should achieve successful integration was identified.
This research employed case study methods to examine the implementation of this policy in two FQHCs in New England. Data were obtained from in-depth interviews with leadership, management, and frontline staff at two case study sites.
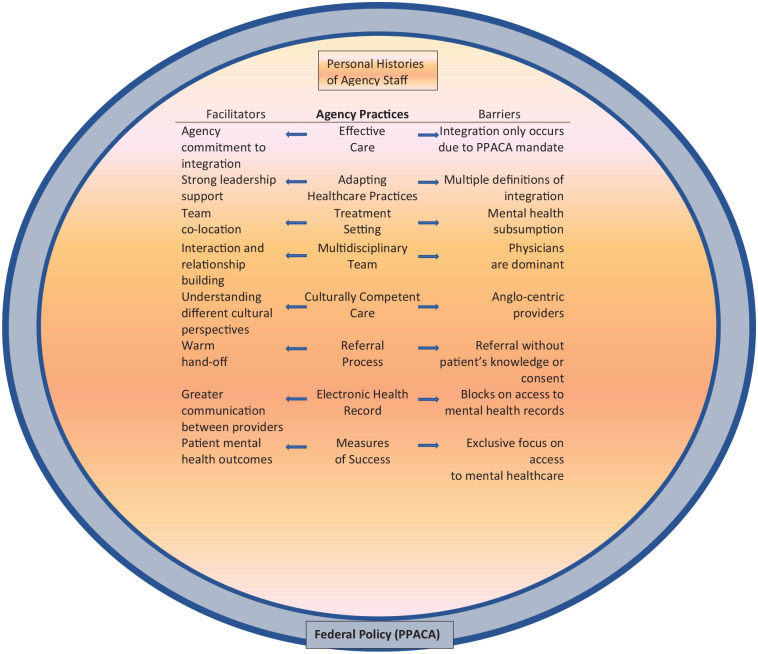
Study findings include multiple definitions of and approaches for integrating physical and mental healthcare, mental healthcare being subsumed into, rather than integrated with, the medical model and multiple facilitators of and barriers to integration.
This study asked questions about what integration means, how it occurs, and what factors facilitate or pose barriers to integration. Integration is facilitated by co-location of providers within the same department, a warm hand-off, collaborative collegial relationships, strong leadership support, and a shared electronic health record. However, interdisciplinary conflict, power differentials, job insecurity, communication challenges, and the subsumption of mental health into the medical model pose barriers to successful integration.
长期以来,在全球范围内有效且适当地提供精神卫生保健一直是一项难题,这导致精神疾病患病率与获得护理的机会之间存在显著差距。为解决这种差距所做的一次尝试是2010年美国的《患者保护与平价医疗法案》(PPACA),该法案要求在联邦合格健康中心(FQHCs)将身体和精神卫生保健整合起来。整合的理念很有吸引力,因为它已显示出改善精神卫生保健可及性和医疗结果的潜力。然而,虽然PPACA法案对FQHCs提出了这一要求,但对于这些中心应如何实现成功整合,却没有明确的流程。
本研究采用案例研究方法,考察了该政策在新英格兰地区两家FQHCs中的实施情况。数据来自对两个案例研究地点的领导、管理层和一线工作人员的深入访谈。
研究结果包括身体和精神卫生保健整合的多种定义和方法、精神卫生保健被纳入而非与医疗模式整合,以及整合的多个促进因素和障碍。
本研究提出了关于整合意味着什么、如何发生以及哪些因素促进或阻碍整合的问题。同一部门内提供者的同址办公、温馨交接、协作的同事关系、强有力的领导支持以及共享的电子健康记录有助于整合。然而,跨学科冲突、权力差异、工作不安全感、沟通挑战以及精神卫生被纳入医疗模式对成功整合构成了障碍。