Leow Jeffrey J, Tan Wei Shen, Tan Wei Phin, Tan Teck Wei, Chan Vinson Wai-Shun, Tikkinen Kari A O, Kamat Ashish, Sengupta Shomik, Meng Maxwell V, Shariat Shahrokh, Roupret Morgan, Decaestecker Karel, Vasdev Nikhil, Chong Yew Lam, Enikeev Dmitry, Giannarini Gianluca, Ficarra Vincenzo, Teoh Jeremy Yuen-Chun
Department of Urology, Tan Tock Seng Hospital, Singapore, Singapore.
Lee Kong Chian School of Medicine, Nanyang Technological University, Singapore, Singapore.
Front Surg. 2022 Oct 4;9:879774. doi: 10.3389/fsurg.2022.879774. eCollection 2022.
The COVID-19 pandemic has led to competing strains on hospital resources and healthcare personnel. Patients with newly diagnosed invasive urothelial carcinomas of bladder (UCB) upper tract (UTUC) may experience delays to definitive radical cystectomy (RC) or radical nephro-ureterectomy (RNU) respectively. We evaluate the impact of delaying definitive surgery on survival outcomes for invasive UCB and UTUC.
We searched for all studies investigating delayed urologic cancer surgery in Medline and Embase up to June 2020. A systematic review and meta-analysis was performed.
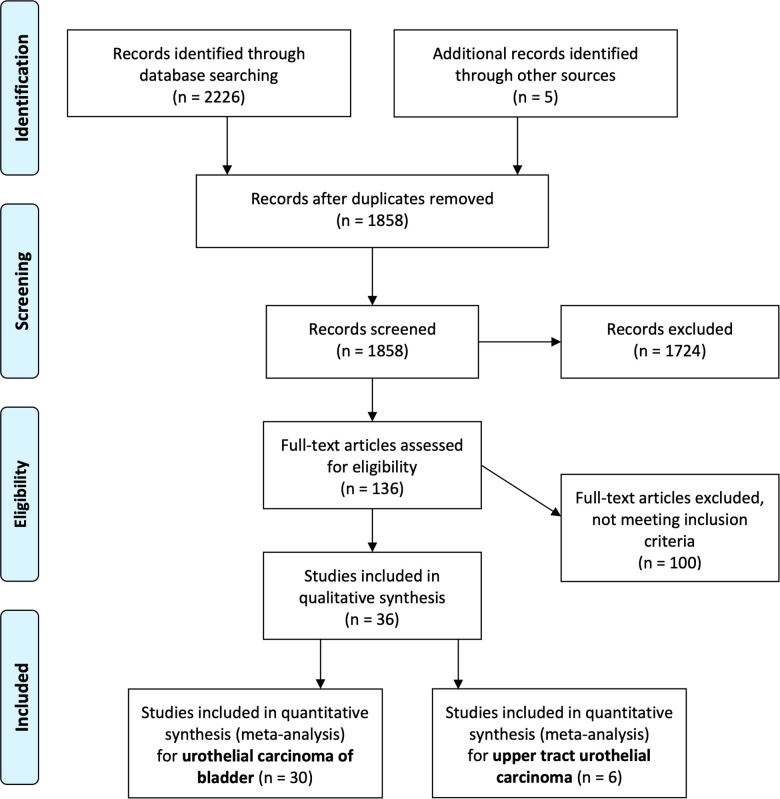
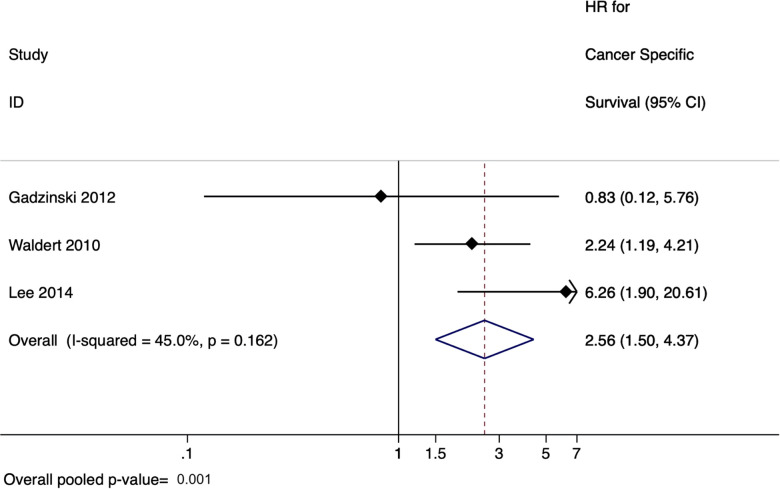
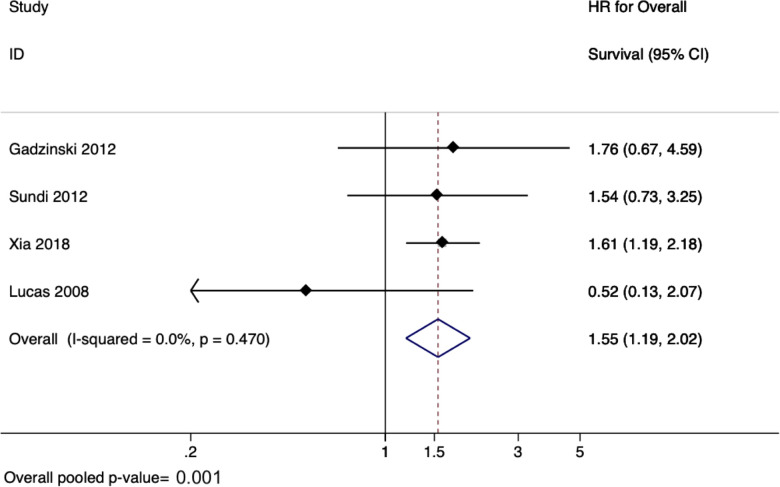
We identified a total of 30 studies with 32,591 patients. Across 13 studies ( = 12,201), a delay from diagnosis of bladder cancer/TURBT to RC was associated with poorer overall survival (HR 1.25, 95% CI: 1.09-1.45, = 0.002). For patients who underwent neoadjuvant chemotherapy before RC, across the 5 studies ( = 4,316 patients), a delay between neoadjuvant chemotherapy and radical cystectomy was not found to be significantly associated with overall survival (pooled HR 1.37, 95% CI: 0.96-1.94, = 0.08). For UTUC, 6 studies ( = 4,629) found that delay between diagnosis of UTUC to RNU was associated with poorer overall survival (pooled HR 1.55, 95% CI: 1.19-2.02, = 0.001) and cancer-specific survival (pooled HR of 2.56, 95% CI: 1.50-4.37, = 0.001). Limitations included between-study heterogeneity, particularly in the definitions of delay cut-off periods between diagnosis to surgery.
A delay from diagnosis of UCB or UTUC to definitive RC or RNU was associated with poorer survival outcomes. This was not the case for patients who received neoadjuvant chemotherapy.
新型冠状病毒肺炎疫情导致医院资源和医护人员面临相互竞争的压力。新诊断为膀胱浸润性尿路上皮癌(UCB)或上尿路尿路上皮癌(UTUC)的患者可能会分别经历根治性膀胱切除术(RC)或根治性肾输尿管切除术(RNU)的延迟。我们评估延迟确定性手术对浸润性UCB和UTUC生存结果的影响。
我们检索了截至2020年6月在Medline和Embase中所有调查延迟泌尿外科癌症手术的研究。进行了系统评价和荟萃分析。
我们共纳入30项研究,涉及32591例患者。在13项研究(n = 12201)中,从膀胱癌诊断/经尿道膀胱肿瘤电切术(TURBT)到RC的延迟与较差的总生存期相关(风险比[HR] 1.25,95%置信区间[CI]:1.09 - 1.45,P = 0.002)。对于在RC前接受新辅助化疗的患者,在5项研究(n = 4316例患者)中,新辅助化疗与根治性膀胱切除术之间的延迟未发现与总生存期有显著关联(合并HR 1.37,95% CI:0.96 - 1.94,P = 0.08)。对于UTUC,6项研究(n = 4629)发现,从UTUC诊断到RNU的延迟与较差的总生存期(合并HR 1.55,95% CI:1.19 - 2.02,P = 0.001)和癌症特异性生存期(合并HR 2.56,95% CI:1.50 - 4.37,P = 0.001)相关。局限性包括研究间的异质性,特别是在诊断到手术的延迟截止期定义方面。
从UCB或UTUC诊断到确定性RC或RNU的延迟与较差的生存结果相关。接受新辅助化疗的患者情况并非如此。