Department of Obstetrics and Gynecology, Fukushima Red Cross Hospital.
Fukushima J Med Sci. 2022 Dec 21;68(3):183-190. doi: 10.5387/fms.2022-23. Epub 2022 Oct 27.
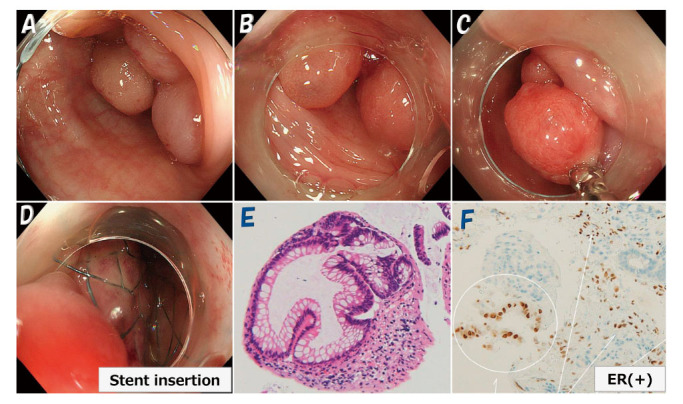
Polypoid endometriosis is a rare form of endometriosis characterized by polypoid masses that histologically often resemble endometrial polyps. We report a case of rapidly progressing polypoid endometriosis that was preoperatively assumed to be advanced ovarian cancer. A 46-year-old woman, para 0, underwent laparoscopic myomectomy and left adnexectomy for uterine fibroids and a left ovarian endometrial cyst after administration of gonadotropin releasing hormone (GnRH) agonist for 4 months. Eleven months postoperatively, rapid right ovarian enlargement occurred. CT and MRI (both contrast-enhanced) showed masses in the right adnexa, cecum, sigmoid colon, and omentum, and PET-CT demonstrated increased uptake, suggesting ovarian cancer and peritoneal dissemination. The patient later developed intestinal obstruction, and colonoscopy revealed multiple polypoid lesions in the sigmoid colon. The omental tumor and right adnexa were biopsied during exploratory laparotomy, and diagnosed as polypoid endometriosis with no malignancy by permanent pathology. The right adnexal tumor shrunk markedly after 4 months of GnRH antagonist treatment. Second laparotomy was then performed for right adnexal tumor resection and ileocecectomy. Pathological examination revealed polypoid endometriosis extending from the ovary to the cecal mucosa. The patient has been asymptomatic for over 1 year postoperatively. The sigmoid colon tumor shrunk but is still present.Polypoid endometriosis predominantly affects the ovaries, colon, peritoneum, and omentum of patients in their 40s and 50s. It is a benign disease but is often difficult to distinguish from malignancy preoperatively because it rapidly forms numerous solid lesions. Although polypoid endometriosis is rare, with no specific imaging findings, including it in a differential diagnosis may facilitate preoperative identification.
息肉状子宫内膜异位症是一种罕见的子宫内膜异位症形式,其特征为息肉状肿块,组织学上常类似于子宫内膜息肉。我们报告一例快速进展的息肉状子宫内膜异位症病例,术前被误诊为晚期卵巢癌。一位 46 岁的妇女,无生育史,因子宫纤维瘤在接受促性腺激素释放激素(GnRH)激动剂治疗 4 个月后接受腹腔镜子宫肌瘤切除术和左侧附件切除术。术后 11 个月,右侧卵巢迅速增大。CT 和 MRI(均增强)显示右侧附件、盲肠、乙状结肠和大网膜有肿块,PET-CT 显示摄取增加,提示卵巢癌和腹膜播散。患者随后出现肠梗阻,结肠镜检查显示乙状结肠有多个息肉样病变。剖腹探查时对大网膜肿瘤和右侧附件进行活检,通过永久性病理检查诊断为息肉状子宫内膜异位症,无恶性肿瘤。右侧附件肿瘤在 GnRH 拮抗剂治疗 4 个月后明显缩小。然后进行第二次剖腹手术,切除右侧附件肿瘤和回盲部切除术。病理检查显示息肉状子宫内膜异位症从卵巢延伸至盲肠黏膜。患者术后 1 年以上无症状。乙状结肠肿瘤缩小但仍存在。息肉状子宫内膜异位症主要影响 40 多岁和 50 多岁患者的卵巢、结肠、腹膜和大网膜。它是一种良性疾病,但由于术前迅速形成大量实性病变,常难以与恶性肿瘤相鉴别。虽然息肉状子宫内膜异位症罕见,无特定的影像学表现,但将其纳入鉴别诊断可能有助于术前识别。