Leng Bing, Shen Chengwu, Gao Tiantian, Zhao Kai, Zhao Xuemei, Guo Yujin, Wu Jiyong, Yang Jing, Fang Wei, Zhang Jicheng, Zhang Yahui, Sun Chao, Duan Lei, Huang Jing, Qi Yougang, Yan Genquan
Department of Pharmacy, Shandong Provincial Hospital Affiliated to Shandong First Medical University, Jinan, China.
Management Office of Information and Network, Shandong Provincial Hospital Affiliated to Shandong First Medical University, Jinan, China.
Front Pharmacol. 2022 Oct 11;13:943674. doi: 10.3389/fphar.2022.943674. eCollection 2022.
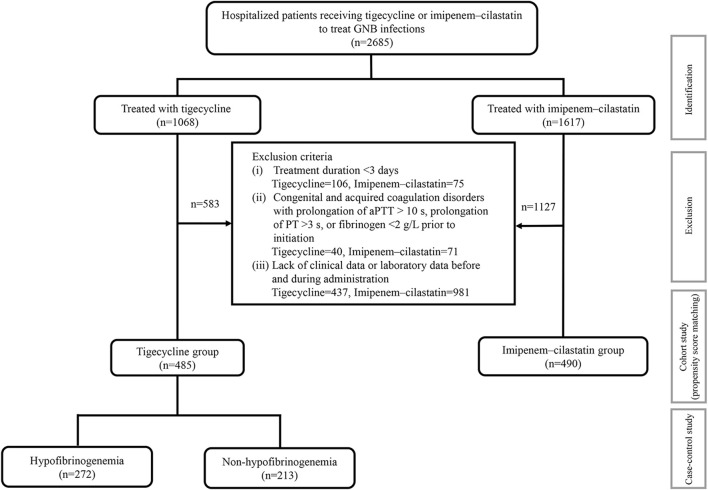
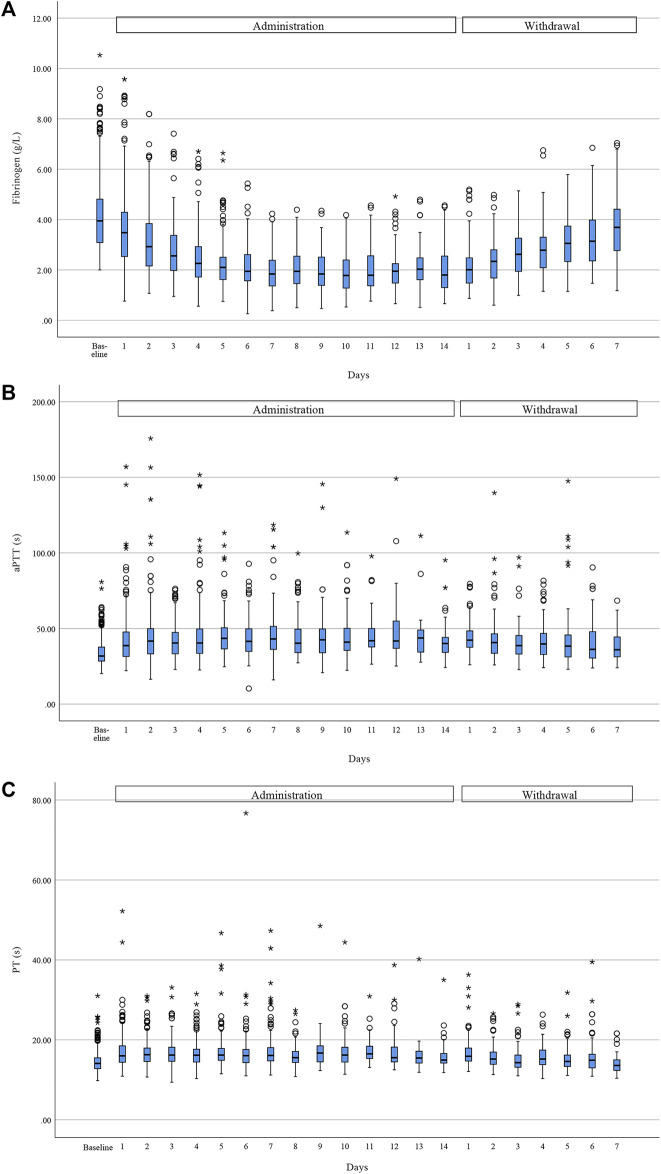
Tigecycline was recently found to cause coagulation disorders, especially hypofibrinogenemia, which may interfere with the administration of antimicrobial therapy. This study aimed to investigate the incidence and clinical characteristics of and risk factors for tigecycline-associated hypofibrinogenemia. In this multicenter retrospective study, patients receiving tigecycline or imipenem-cilastatin to treat Gram-negative bacterial infections in nine Chinese tertiary hospitals between January 2020 and December 2020 were enrolled. Baseline data and coagulation variables were compared using cohort and case-control studies. Totals of 485 patients treated with tigecycline and 490 patients treated with imipenem-cilastatin were included in this study. Compared with imipenem-cilastatin, tigecycline was associated with reduced fibrinogen and prolonged activated partial thromboplastin time and prothrombin time (all < 0.001), with the most remarkable change in fibrinogen (down by 48.0%). The incidence of hypofibrinogenemia in patients treated with tigecycline was >50%, with propensity score-matched analysis or not. The relative risk of hypofibrinogenemia with tigecycline versus imipenem-cilastatin was 2.947 (95% CI: 2.151-4.039) at baseline balance. Tigecycline-associated hypofibrinogenemia led to a higher incidence (12.1%) of bleeding events. However, none of supplemental therapies after withdrawal had an effect on the normalization of fibrinogen levels. The risk factors for tigecycline-associated hypofibrinogenemia were treatment duration ≥6 days (odds ratio [OR] 5.214, 95% confidence interval [CI] 2.957-9.191, < 0.001), baseline fibrinogen <4 g/L (OR 4.625, 95% CI 2.911-7.346, < 0.001), cumulative dose ≥1,000 mg (OR 2.637, 95% CI 1.439-4.832, = 0.002), receiving CRRT (OR 2.436, 95% CI 1.179-5.031, = 0.016), baseline PT > 14 s (OR 2.110, 95% CI 1.317-3.380, = 0.002) and baseline total bilirubin >21 μmol/L (OR 1.867, 95% CI 1.107-3.147, = 0.019), while the protective factor was skin and soft tissue infection (OR 0.110, 95% CI 0.026-0.473, = 0.003). The clinical characteristics of and risk factors for tigecycline-associated hypofibrinogenemia identified in this study can offer practical reference for the clinical management of patients.
替加环素最近被发现可导致凝血障碍,尤其是低纤维蛋白原血症,这可能会干扰抗菌治疗的实施。本研究旨在调查替加环素相关低纤维蛋白原血症的发生率、临床特征及危险因素。在这项多中心回顾性研究中,纳入了2020年1月至2020年12月期间在9家中国三级医院接受替加环素或亚胺培南 - 西司他丁治疗革兰阴性菌感染的患者。使用队列研究和病例对照研究比较基线数据和凝血变量。本研究共纳入485例接受替加环素治疗的患者和490例接受亚胺培南 - 西司他丁治疗的患者。与亚胺培南 - 西司他丁相比,替加环素与纤维蛋白原降低、活化部分凝血活酶时间和凝血酶原时间延长相关(均P<0.001),其中纤维蛋白原变化最为显著(下降48.0%)。无论是否进行倾向评分匹配分析,接受替加环素治疗的患者低纤维蛋白原血症的发生率均>50%。在基线平衡时,替加环素与亚胺培南 - 西司他丁相比,低纤维蛋白原血症的相对风险为2.947(95%CI:2.151 - 4.039)。替加环素相关低纤维蛋白原血症导致出血事件的发生率较高(12.1%)。然而,停药后的补充治疗均未对纤维蛋白原水平恢复正常产生影响。替加环素相关低纤维蛋白原血症的危险因素包括治疗持续时间≥6天(比值比[OR]5.214,95%置信区间[CI]2.957 - 9.191,P<0.001)、基线纤维蛋白原<4g/L(OR 4.625,95%CI 2.911 - 7.346,P<0.001)、累积剂量≥1000mg(OR 2.637,95%CI 1.439 - 4.83e,P = 0.002)、接受连续性肾脏替代治疗(CRRT)(OR 2.436,95%CI 1.179 - 5.031,P = 0.016)、基线凝血酶原时间>14秒(OR 2.110,95%CI 1.317 - 3.380,P = 0.002)和基线总胆红素>21μmol/L(OR 1.867,95%CI 1.107 - 3.147,P = 0.019),而保护因素是皮肤和软组织感染(OR 0.110,95%CI 0.026 - 0.473,P = 0.003)。本研究中确定的替加环素相关低纤维蛋白原血症的临床特征和危险因素可为患者的临床管理提供实际参考。