Vanderbilt University School of Medicine, Nashville, TN, USA.
Division of Interventional Radiology, Vanderbilt University Medical Center, CCC-1118 Medical Center North, 1161 21st Ave S, Nashville, TN, 37232, USA.
BMC Gastroenterol. 2022 Nov 17;22(1):467. doi: 10.1186/s12876-022-02528-y.
National Comprehensive Cancer Network HCC guidelines recommend Y90 to treat BCLC-C patients only in select cases given the development of systemic regimens. We sought to identify ideal candidates for Y90 by assessing survival and toxicities in this patient group.
The Radiation-Emitting Selective Internal radiation spheres in Non-resectable tumor registry is a prospective observational study (NCT: 02,685,631). Patients with advanced HCC were stratified into 3 groups based on tumor location, Eastern Cooperative Oncology Group (ECOG) performance status, and liver function. Group 1: liver isolated HCC, ECOG 0 and Child Pugh (CP) A (n = 12, 16%), Group 2: liver isolated HCC, ECOG ≥ 1 or CP B/C (n = 37, 49%), and Group 3: extrahepatic HCC with any ECOG or CP score (n = 26, 35%). Patients in any group could have macrovascular invasion. Overall survival (OS) and progression-free survival (PFS) with 95% confidence intervals (95% CI) were calculated. Grade 3 + toxicities were tracked using Common Terminology Criteria for Adverse Events v5. Cox proportional hazard model was performed to determine factors affecting OS.
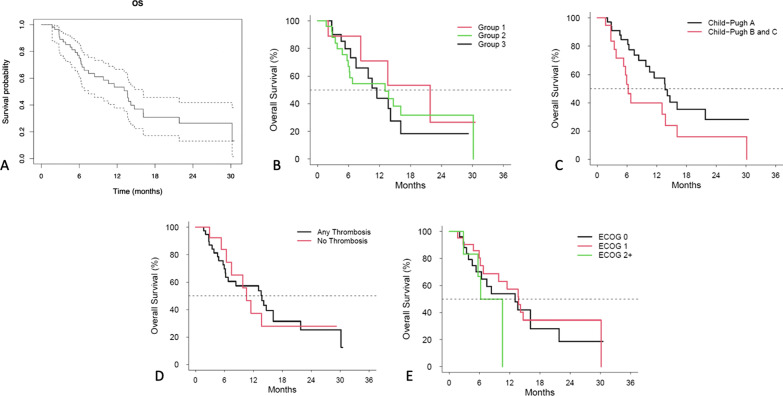
Seventy-five BCLC-C patients treated between 2015 and 2019 were reviewed. The groups were similar in age, sex, race, and ethnicity (all p > 0.05). Bilobar disease was least common in Group 1 (p < 0.001). Median OS of the entire cohort was 13.6 (95% CI 7.5-16.1) months. Median OS of Groups 1-3 were 21.8, 13.1 and 11.5 months respectively (p = 0.6). Median PFS for the cohort was 6.3 (4.8-14.7) months. Median PFS for group 1 was not reached. Mean PFS for Group 1 was 17.3 ± 4.8 months. Median PFS for Groups 2 and 3 was 6.8 and 5.9 months (X = 1.5, p = 0.5). Twenty-four Grade 3 or greater toxicities developed, most commonly hyperbilirubinemia (8/75, 11%) and thrombocytopenia (2/75, 3%). The incidence of toxicities between groups was similar (all p > 0.05). Cox Proportional Hazard analysis predicted shorter OS with CP class B/C (X = 6.7, p = 0.01), while macrovascular invasion (X = 0.5, p = 0.5) and ECOG score of ≥ 1 (X = 2.1, p = 0.3) was not associated with OS.
OS of CPA patients with advanced HCC and performance status of 0 was 21.8 months following Y90. CP A cirrhosis is the best predictor of prolonged OS in advanced (BCLC-C) HCC.
美国国家综合癌症网络 HCC 指南建议 Y90 仅用于治疗特定情况下的 BCLC-C 患者,因为已经开发了全身治疗方案。我们通过评估该患者群体的生存和毒性,旨在确定 Y90 的理想候选者。
不可切除肿瘤登记处的放射性发射选择性内部辐射球体是一项前瞻性观察性研究(NCT:02,685,631)。根据肿瘤位置、东部合作肿瘤学组(ECOG)表现状态和肝功能,将晚期 HCC 患者分为 3 组。第 1 组:孤立性肝癌,ECOG 0 和 Child Pugh(CP)A(n=12,16%);第 2 组:孤立性肝癌,ECOG≥1 或 CP B/C(n=37,49%);第 3 组:有任何 ECOG 或 CP 评分的肝外 HCC(n=26,35%)。任何组的患者都可能有大血管侵犯。计算了总生存期(OS)和无进展生存期(PFS)的 95%置信区间(95%CI)。使用常见不良事件术语标准 5.0(CTCAE v5.0)跟踪 3+级毒性。使用 Cox 比例风险模型确定影响 OS 的因素。
回顾了 2015 年至 2019 年期间治疗的 75 例 BCLC-C 患者。各组在年龄、性别、种族和民族方面相似(均 p>0.05)。第 1 组中双侧疾病最少见(p<0.001)。整个队列的中位 OS 为 13.6(95%CI 7.5-16.1)个月。第 1-3 组的中位 OS 分别为 21.8、13.1 和 11.5 个月(p=0.6)。该队列的中位 PFS 为 6.3(4.8-14.7)个月。第 1 组的中位 PFS 未达到。第 1 组的平均 PFS 为 17.3±4.8 个月。第 2 组和第 3 组的中位 PFS 分别为 6.8 和 5.9 个月(X=1.5,p=0.5)。24 例出现 3 级或更高级别的毒性,最常见的是高胆红素血症(8/75,11%)和血小板减少症(2/75,3%)。各组之间的毒性发生率相似(均 p>0.05)。Cox 比例风险分析预测 CP 类 B/C 患者的 OS 更短(X=6.7,p=0.01),而大血管侵犯(X=0.5,p=0.5)和 ECOG 评分≥1(X=2.1,p=0.3)与 OS 无关。
Y90 治疗后,CP A 肝硬化的晚期 HCC 患者和表现状态为 0 的患者的 OS 为 21.8 个月。CP A 肝硬化是预测晚期(BCLC-C)HCC 患者 OS 延长的最佳指标。