Asif Talal, Doukky Rami
Division of Cardiology, University Health Truman Medical Center, 2301 Holmes Street, Kansas City, MO 64108, USA.
Division of Cardiology, Cook County Health, 1969 W Ogden Ave, Chicago, IL 60612, USA.
Radiol Case Rep. 2022 Nov 25;18(2):538-544. doi: 10.1016/j.radcr.2022.11.006. eCollection 2023 Feb.
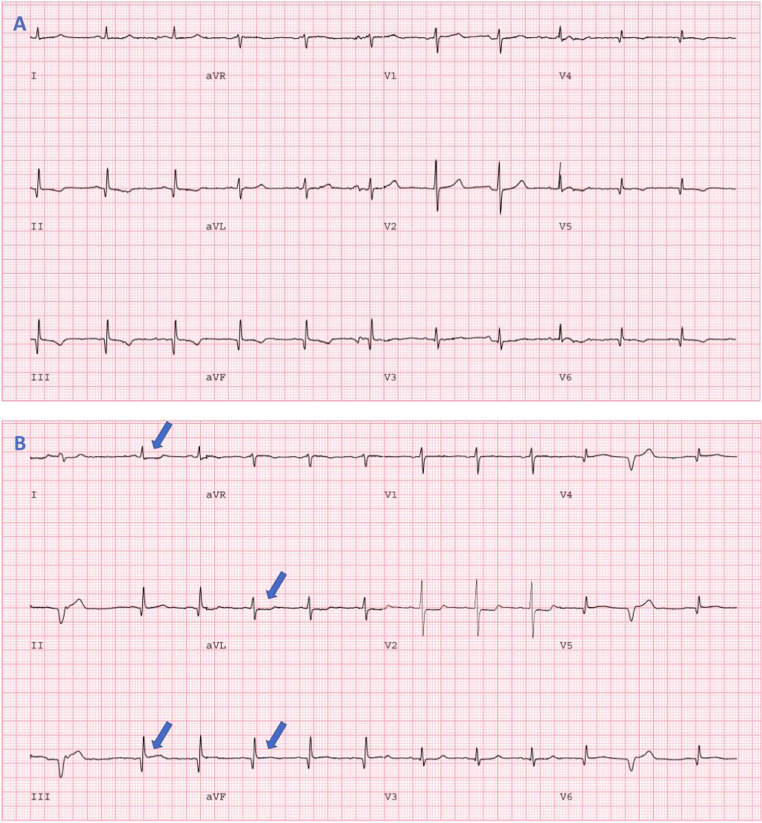
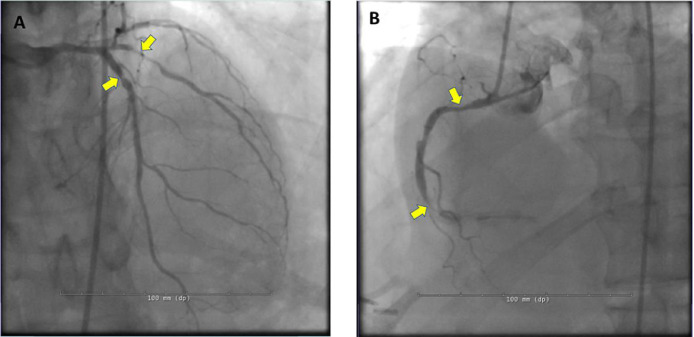
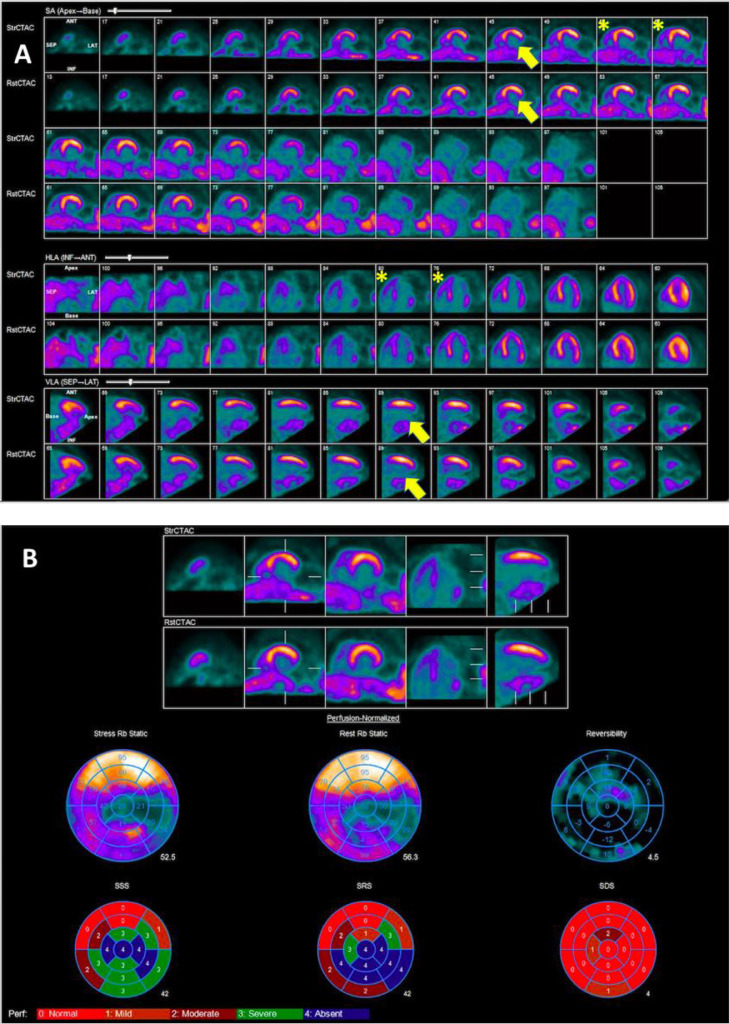
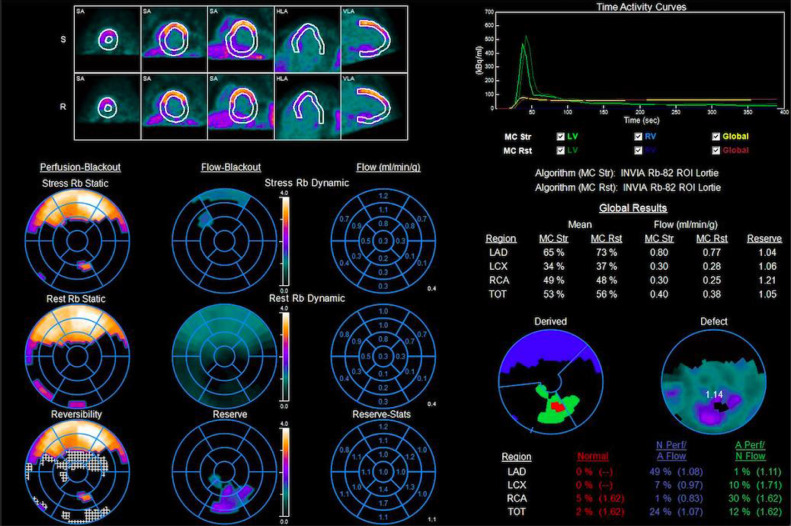
Myocardial perfusion imaging (MPI) with single photon emission computed tomography (SPECT) or positron emission tomography (PET) is a widely used technique for the evaluation of coronary artery disease (CAD). Interpreting physicians rely on regional variations in myocardial radiotracer uptake between rest and stress images to identify hemodynamically significant epicardial coronary artery stenosis. However, interpretation of MPI is very difficult in patients with large infarcts where there is no scintigraphically normal reference myocardium for comparison. In these patients, the stress and rest images appear similar due to balanced ischemia in the non-infarct territory. There are no clear guidelines on how to approach these cases. We present a case of MPI with a large right coronary artery territory (RCA) infarct where the left main (LM) coronary artery territory has no relative comparator and the images looked the same on stress and rest. However, the patient had multiple high-risk ancillary findings including electrocardiographic (ECG) changes with regadenoson, transient ischemic dilatation (TID), large severe inferior infarct, low myocardial blood flow (MBF) and myocardial flow reserve (MFR), but most notably increased right ventricular (RV) uptake on the stress images that was a subtle clue that we were dealing with LM equivalent in non-infarct zone. The coronary angiogram confirmed our findings. Through our case, we provide a comprehensive approach and review of literature on how to approach such challenging encounters.
使用单光子发射计算机断层扫描(SPECT)或正电子发射断层扫描(PET)进行心肌灌注成像(MPI)是一种广泛用于评估冠状动脉疾病(CAD)的技术。解读医生依靠静息和负荷图像中心肌放射性示踪剂摄取的区域差异来识别具有血流动力学意义的心外膜冠状动脉狭窄。然而,对于大面积梗死患者,MPI的解读非常困难,因为没有闪烁显像正常的参照心肌进行比较。在这些患者中,由于非梗死区域存在平衡缺血,负荷和静息图像看起来相似。目前尚无关于如何处理这些病例的明确指南。我们报告一例右冠状动脉区域(RCA)大面积梗死的MPI病例,其中左主干(LM)冠状动脉区域没有相对参照,且负荷和静息图像看起来相同。然而,该患者有多个高危辅助检查结果,包括使用雷加昔布时的心电图(ECG)变化、短暂性缺血性扩张(TID)、大面积严重下壁梗死、低心肌血流量(MBF)和心肌血流储备(MFR),但最显著的是负荷图像上右心室(RV)摄取增加,这是一个微妙线索,提示我们在非梗死区域处理的是等同于LM的情况。冠状动脉造影证实了我们的发现。通过我们的病例,我们提供了一种全面的方法,并对如何处理此类具有挑战性的情况的文献进行了综述。