Cardiac Surgery Department, Fundación Cardioinfantil-Institute of Cardiology, Rosario University, Calle 163 A # 13B-60, 111831, Bogotá, Colombia.
Cardiothoracic surgery, Hospital universitario mayor MEDERI, Bogotá, Colombia.
J Cardiothorac Surg. 2022 Dec 29;17(1):341. doi: 10.1186/s13019-022-02058-4.
The lack of evidence on complications using mitral valve approaches leaves the choice of risk exposure to the surgeon's preference, based on individual experience, speed, ease, and quality of exposure.
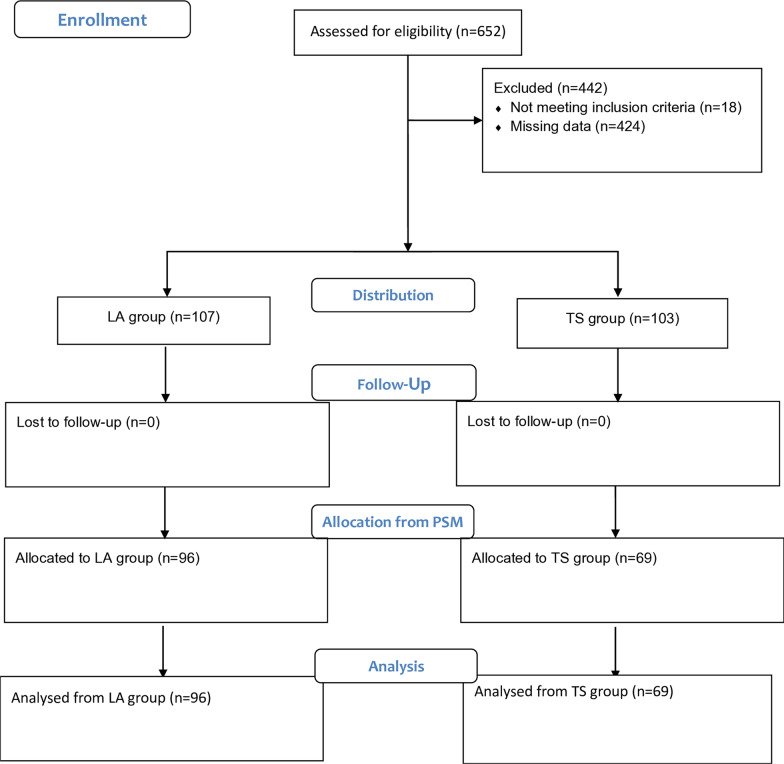
The present study analysed patients undergoing mitral valve surgery using a superior transseptal approach or a left-atrial approach between 2006 and 2018. We included first-time elective mitral valve procedures, isolated, or combined, without a history of rhythm disturbances. We used propensity score matching based on 26 perioperative variables. The primary endpoint was the association between the superior transeptal approach and clinically significant adverse outcomes, including arrhythmias, need for a permanent pacemaker, cerebrovascular events, and mortality.
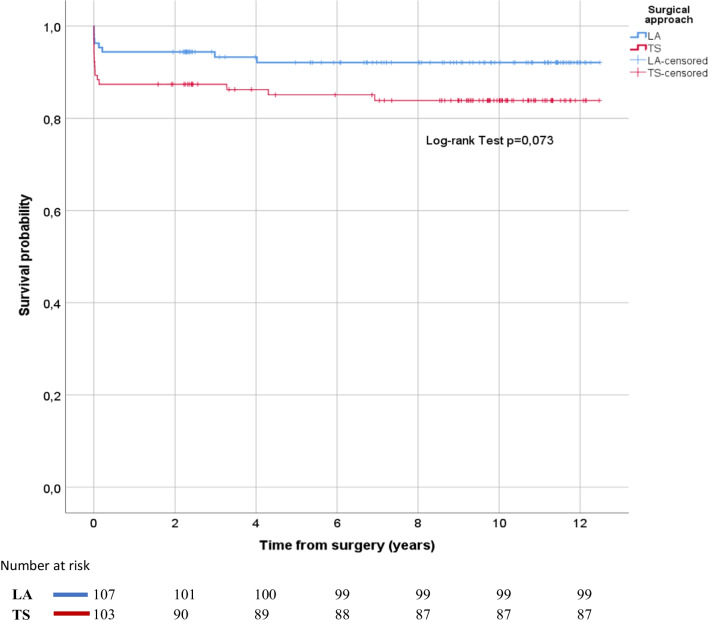
A total of 652 patients met the inclusion criteria; 391 received the left atrial approach, and 261 received the superior transseptal approach. After matching, 96 patients were compared with 69 patients, respectively. The distribution of the preoperative and perioperative variables was similar. There was no difference in the incidence of supraventricular tachyarrhythmias or the need for treatment. The incidence of nodal rhythm (p = 0.008) and length of stay in intensive care (p = 0.04) were higher in the superior transseptal group, but the need for permanent pacemaker implantation was the same. Likewise, there was no difference in the need for anticoagulation due to arrhythmia, the incidence of cerebrovascular events or mortality in the postoperative period or in the long-term follow-up.
We did not find an association with permanent heart rhythm disorders or any other significant adverse clinical outcome. Therefore, the superior transeptal approach is useful and safe for mitral valve exposure.
由于缺乏使用二尖瓣入路的并发症证据,风险暴露的选择取决于外科医生的偏好,基于个人经验、速度、难易程度和显露质量。
本研究分析了 2006 年至 2018 年间接受经上腔静脉入路或左心房入路二尖瓣手术的患者。我们纳入了首次择期二尖瓣手术,包括单纯或联合手术,且无节律紊乱病史。我们使用基于 26 个围手术期变量的倾向评分匹配。主要终点是上腔静脉入路与心律失常、永久性起搏器需求、脑血管事件和死亡率等临床显著不良结局之间的关联。
共有 652 名患者符合纳入标准;391 名患者接受了左心房入路,261 名患者接受了上腔静脉入路。匹配后,分别比较了 96 例和 69 例患者。术前和围手术期变量的分布相似。房性心动过速或治疗需求的发生率无差异。上腔静脉入路组窦性节律(p=0.008)和重症监护病房停留时间(p=0.04)的发生率较高,但永久性起搏器植入的需求相同。同样,心律失常导致抗凝的需求、术后或长期随访期间的脑血管事件或死亡率无差异。
我们没有发现永久性心脏节律紊乱或任何其他重大不良临床结局的关联。因此,上腔静脉入路用于二尖瓣显露是有用且安全的。