Department of Neonatology, Women and Children's Hospital, School of Medicine, Xiamen University, Xiamen, 361003, Fujian, China.
Xiamen Key Laboratory of Perinatal-Neonatal Infection, Xiamen, China.
Ital J Pediatr. 2023 Jan 26;49(1):14. doi: 10.1186/s13052-023-01414-x.
Infants with rule-out infections are responsible for the majority of empirical antibiotics treatment (EAT) in neonatal intensive care units (NICUs), particularly very preterm infants (VPIs). Antibiotic overuse has been linked to adverse outcomes. There is a paucity of data on the association between EAT and clinical outcomes (containing the nutritional outcomes) of VPIs without infection-related morbidities.
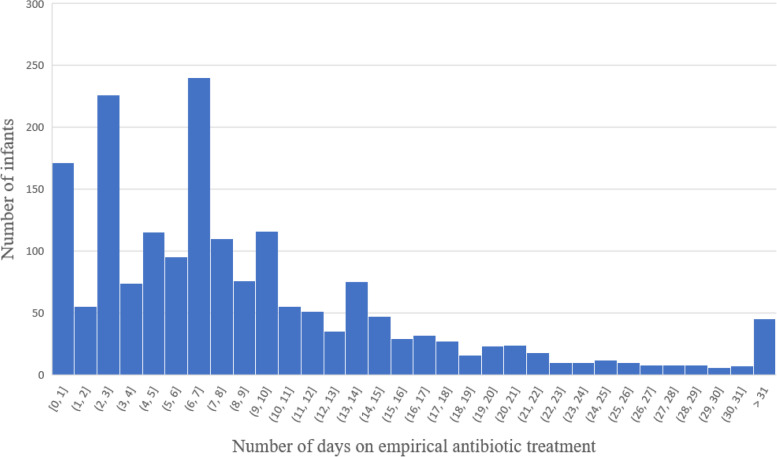
Clinical data of VPIs admitted in 28 hospitals in 20 provinces of China from September 2019 to December 2020 were collected. EAT of VPIs was calculated as the number of days with initial usage in the first week after birth, and then categorized into 3 groups (antibiotic exposure: none, 1-4 days, and > 4 days). Clinical characteristics, nutritional status , and the short-term clinical outcomes among 3 groups were compared and analyzed.
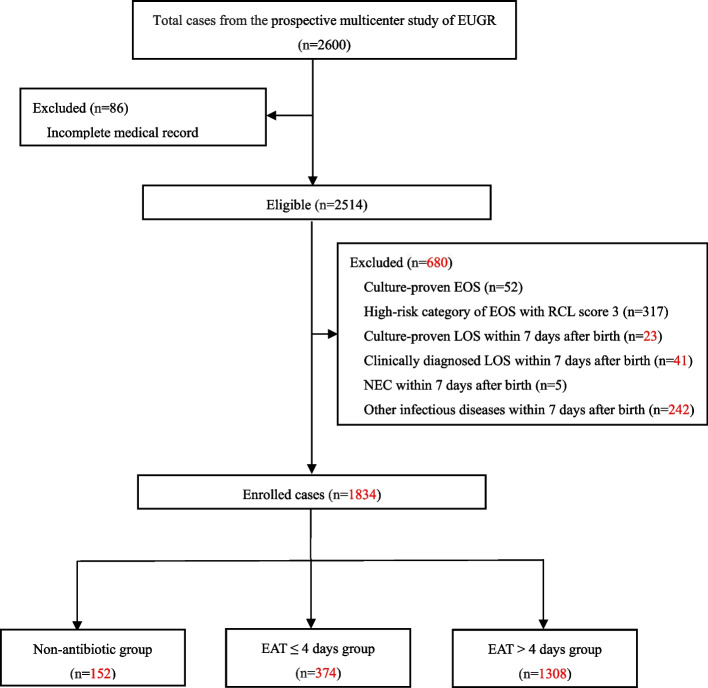
In total, 1834 VPIs without infection-related morbidities in the first postnatal week were enrolled, including 152 cases (8.3%) without antibiotics, 374 cases (20.4%) with EAT ≤4 days and 1308 cases (71.3%) with EAT > 4 days. After adjusting for the confounding variables, longer duration of EAT was associated with decreased weight growth velocity and increased duration of reach of full enteral feeding in EAT > 4 days group (aβ: -4.83, 95% CI: - 6.12 ~ - 3.53; aβ: 2.77, 95% CI: 0.25 ~ 5.87, respectively) than those receiving no antibiotics. In addition, the risk of feeding intolerance (FI) in EAT > 4 days group was 4 times higher than that in non-antibiotic group (aOR: 4.14, 95%CI: 1.49 ~ 13.56) and 1.8 times higher than that in EAT ≤4 days group (aOR: 1.82, 95%CI: 1.08 ~ 3.17). EAT > 4 days was also a risk factor for greater than or equal to stage 2 necrotizing enterocolitis (NEC) than those who did not receive antibiotics (aOR: 7.68, 95%CI: 1.14 ~ 54.75) and those who received EAT ≤4 days antibiotics (aOR: 5.42, 95%CI: 1.94 ~ 14.80).
The EAT rate among uninfected VPIs was high in Chinese NICUs. Prolonged antibiotic exposure was associated with decreased weight growth velocity, longer duration of reach of full enteral feeding, increased risk of feeding intolerance and NEC ≥ stage 2. Future stewardship interventions to reduce EAT use should be designed and implemented.
在新生儿重症监护病房(NICU)中,排除感染的婴儿是接受经验性抗生素治疗(EAT)的主要人群,尤其是非常早产儿(VPIs)。抗生素的过度使用与不良结局有关。目前关于无感染相关并发症的 VPI 接受 EAT 与临床结局(包括营养结局)之间的关联的数据很少。
收集了 2019 年 9 月至 2020 年 12 月中国 28 家医院的 1834 例无感染相关并发症的 VPI 临床数据。VPIs 的 EAT 计算为出生后第一周初始使用的天数,并分为 3 组(抗生素暴露:无、1-4 天和>4 天)。比较和分析了 3 组间的临床特征、营养状况和短期临床结局。
共纳入了 1834 例出生后第一周无感染相关并发症的 VPI,其中 152 例(8.3%)无抗生素,374 例(20.4%)EAT≤4 天,1308 例(71.3%)EAT>4 天。调整混杂变量后,EAT 持续时间较长与 EAT>4 天组的体重增长速度下降和完全肠内喂养时间延长有关(aβ:-4.83,95%CI:-6.12-3.53;aβ:2.77,95%CI:0.255.87),而不是未接受抗生素的组。此外,EAT>4 天组喂养不耐受(FI)的风险是未接受抗生素组的 4 倍(aOR:4.14,95%CI:1.4913.56),是 EAT≤4 天组的 1.8 倍(aOR:1.82,95%CI:1.083.17)。EAT>4 天也比未接受抗生素(aOR:7.68,95%CI:1.1454.75)和 EAT≤4 天抗生素(aOR:5.42,95%CI:1.9414.80)的婴儿发生≥2 级坏死性小肠结肠炎(NEC)的风险更高。
中国 NICU 中无感染的 VPI 接受 EAT 的比例较高。延长抗生素暴露与体重增长速度下降、完全肠内喂养时间延长、喂养不耐受和 NEC≥2 级的风险增加有关。应设计和实施减少 EAT 使用的管理干预措施。