Department of Infectious Disease, The Second Hospital of Nanjing, School of Public Health, Nanjing Medical University, Nanjing, China.
Department of Infectious Disease, The Second Hospital of Nanjing, Nanjing University of Chinese Medicine, Nanjing, China.
Front Immunol. 2023 Jan 9;13:1033098. doi: 10.3389/fimmu.2022.1033098. eCollection 2022.
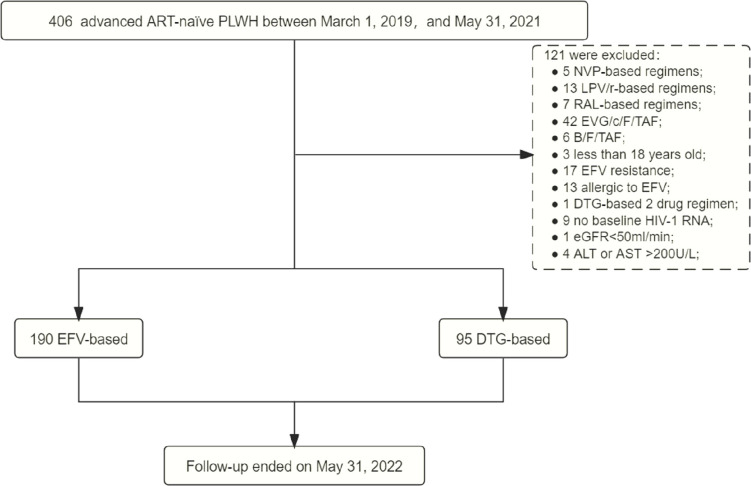
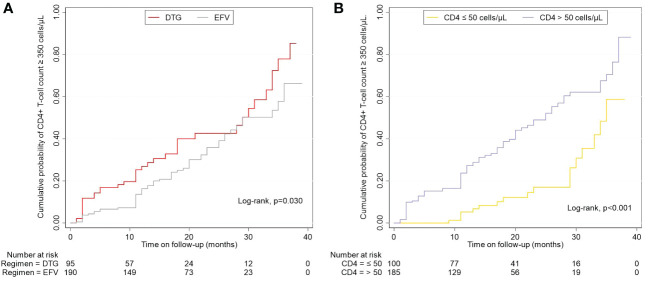
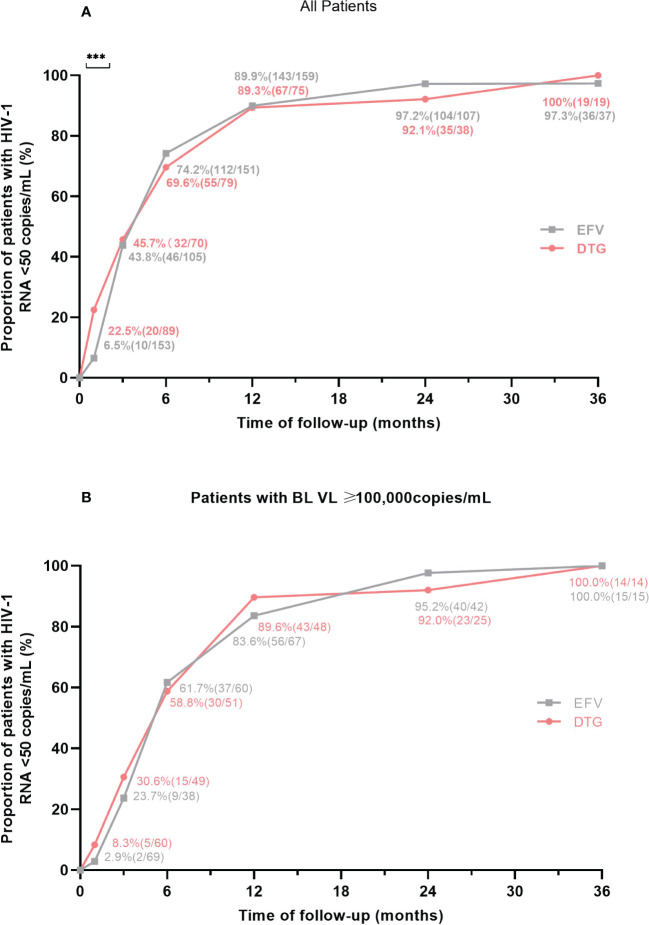
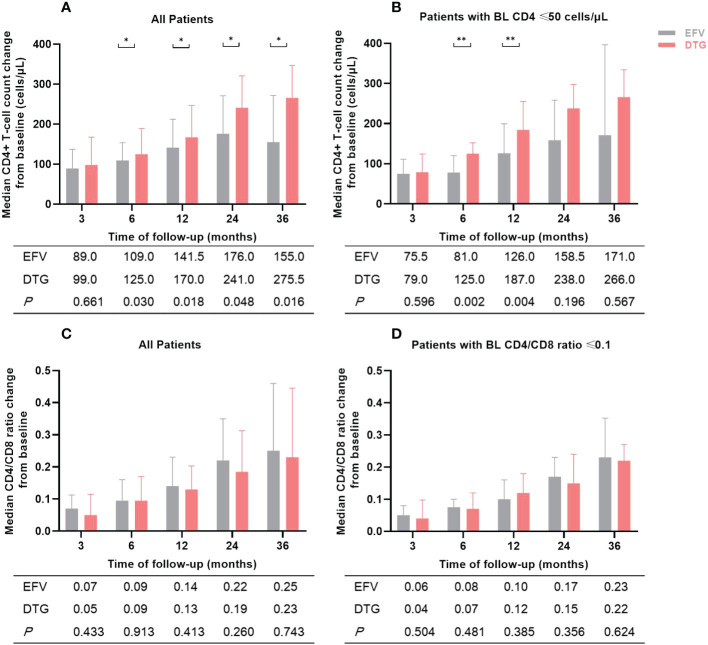
Currently, there are limited data related to the efficacy and safety of ART regimens, as well as factors influencing immune recovery in antiretroviral therapy (ART)-naïve patients with advanced HIV infection, especially in China. We designed a single-center, retrospective cohort study from March 1, 2019, to May 31, 2022, at The Second Hospital of Nanjing, China. ART-naïve adults with advanced HIV infection (CD4+ T-cell count < 200 cells/μL) who met the study criteria were included. The plasma viral load (VL), CD4+ T-cell count, CD4/CD8 ratio, treatment discontinuation, and immune reconstitution inflammatory syndrome (IRIS) events were collected to compare the efficacy and safety of the dolutegravir (DTG) and the efavirenz (EFV) regimens. Factors of immune recovery were analyzed using the Cox regression model. Study enrolled 285 ART-naïve adults with advanced HIV-1 infection, of which 95 (33.3%) started regimens including DTG and 190 (66.7%) were treated with EFV. After ART initiation, the proportion of patients with HIV-1 RNA < 50 copies/mL was higher (22.5% versus 6.5%, < 0.001) in those on DTG-based regimens at month 1, but no significant difference at other follow-up points. Compared to the baseline, the median CD4+ T-cell count and CD4/CD8 ratio increased significantly during follow-up both in the EFV and the DTG groups. However, the CD4+ T-cell count increased greater in patients on DTG-based regimens at months 6, 12, 24, and 36 ( < 0.05). A total of 52 (18.2%) patients discontinued treatment, with no significant difference between ART regimens in treatment discontinuation rates. Only 7 patients reported IRIS, without significant difference between ART regimens (=0.224). Overall, 34.0% (97/285) achieved a CD4+ T-cell count ≥ 350 cells/μL during follow-up. Age ( < 0.001), baseline CD4+ T-cell count ( < 0.001), baseline VL ( < 0.001) and ART regimens ( = 0.019) were associated with the CD4+ T-cell count ≥ 350 cells/μL after adjusting for potential confounders. Among ART-naïve adults with advanced HIV infection, it appeared that DTG-based regimens were better options for initial therapy compared to regimens including EFV; in addition, ART regimens, age, baseline VL and CD4+ T-cell count were associated with immune recovery.
目前,关于抗逆转录病毒治疗(ART)初治的晚期 HIV 感染患者的 ART 方案疗效和安全性,以及影响免疫恢复的因素的数据有限,特别是在中国。我们设计了一项单中心、回顾性队列研究,于 2019 年 3 月 1 日至 2022 年 5 月 31 日在南京第二医院进行。符合研究标准的晚期 HIV 感染(CD4+T 细胞计数<200 个/μL)的 ART 初治成人被纳入研究。收集血浆病毒载量(VL)、CD4+T 细胞计数、CD4/CD8 比值、治疗停药和免疫重建炎症综合征(IRIS)事件,以比较多替拉韦(DTG)和依非韦伦(EFV)方案的疗效和安全性。使用 Cox 回归模型分析免疫恢复的因素。研究纳入了 285 名晚期 HIV-1 感染的 ART 初治成人,其中 95 名(33.3%)开始使用 DTG 方案,190 名(66.7%)接受 EFV 治疗。在开始 ART 后,在第 1 个月时,基于 DTG 方案的患者中 HIV-1 RNA<50 拷贝/mL 的比例更高(22.5%比 6.5%,<0.001),但在其他随访点没有显著差异。与基线相比,EFV 和 DTG 组在随访期间的 CD4+T 细胞计数和 CD4/CD8 比值均显著增加。然而,基于 DTG 的方案在第 6、12、24 和 36 个月时的 CD4+T 细胞计数增加更大(<0.05)。共有 52 名(18.2%)患者停药,ART 方案之间的停药率无显著差异。只有 7 名患者报告了 IRIS,ART 方案之间无显著差异(=0.224)。总的来说,在随访期间,有 34.0%(97/285)的患者达到了 CD4+T 细胞计数≥350 个/μL。年龄(<0.001)、基线 CD4+T 细胞计数(<0.001)、基线 VL(<0.001)和 ART 方案(=0.019)是在调整潜在混杂因素后与 CD4+T 细胞计数≥350 个/μL 相关的因素。在晚期 HIV 感染的 ART 初治成人中,与包含 EFV 的方案相比,基于 DTG 的方案似乎是初始治疗的更好选择;此外,ART 方案、年龄、基线 VL 和 CD4+T 细胞计数与免疫恢复相关。