Department of Family Practice (Stoll), University of British Columbia; Provincial Health Services Authority (Titoria); Midwifery Program (Turner, Butska), Department of Family Practice, University of British Columbia; Women's Health Research Institute (Jones), BC Women's Hospital, Vancouver, BC
Department of Family Practice (Stoll), University of British Columbia; Provincial Health Services Authority (Titoria); Midwifery Program (Turner, Butska), Department of Family Practice, University of British Columbia; Women's Health Research Institute (Jones), BC Women's Hospital, Vancouver, BC.
CMAJ. 2023 Feb 27;195(8):E292-E299. doi: 10.1503/cmaj.220453.
Anecdotal evidence suggests that the profile of midwifery clients in British Columbia has changed over the past 20 years and that midwives are increasingly caring for clients with moderate to high medical risk. We sought to compare perinatal outcomes with a registered midwife as the most responsible provider (MRP) versus outcomes among clients with physicians as their MRP across medical risk strata.
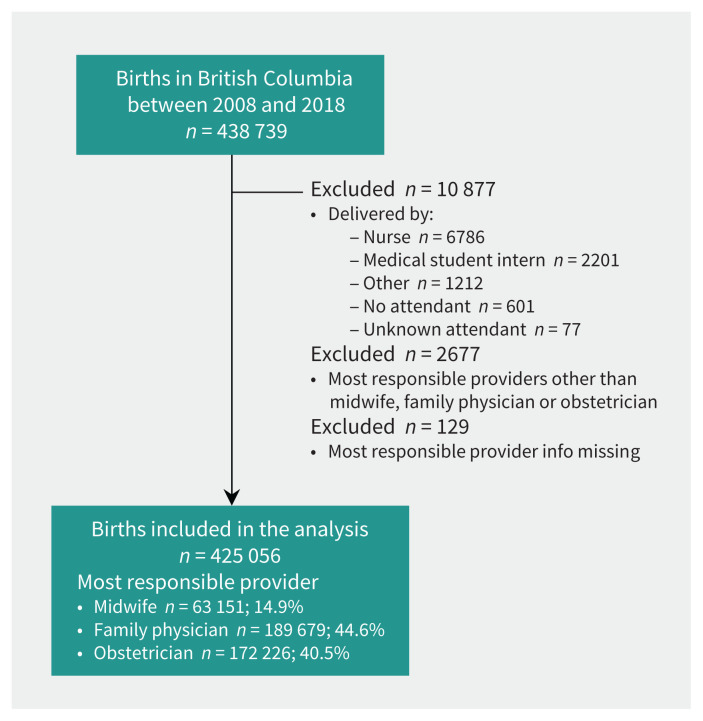
This retrospective cohort study (2008-2018) used data from the BC Perinatal Data Registry. We included all births that had a family physician, obstetrician or midwife listed as the MRP ( = 425 056) and stratified the analysis by pregnancy risk status (low, moderate or high) according to an adapted perinatal risk scoring system. We estimated differences in outcomes between MRP groups by calculating adjusted absolute and relative risks.
The adjusted absolute and relative risks of adverse neonatal outcomes were consistently lower among those who chose midwifery care across medical risk strata, compared with clients who had a physician as MRP. Midwifery clients experienced higher rates of spontaneous vaginal births, vaginal births after cesarean delivery and breastfeeding initiation, and lower rates of cesarean deliveries and instrumental births, with no increase in adverse neonatal outcomes. We observed an increased risk of oxytocin induction among high-risk birthers with a midwife versus an obstetrician as MRP.
Our findings suggest that compared with other providers in BC, midwives provide safe primary care for clients with varied levels of medical risk. Future research might examine how different practice and remuneration models affect clinical outcomes, client and provider experiences, and costs to the health care system.
有传闻证据表明,在过去的 20 年中,不列颠哥伦比亚省的助产士客户群体发生了变化,并且助产士越来越多地照顾具有中等到高医疗风险的客户。我们试图比较有注册助产士作为主要责任提供者(MRP)与医生作为 MRP 的客户在各个医疗风险阶层的围产儿结局。
这项回顾性队列研究(2008-2018 年)使用了不列颠哥伦比亚省围产期数据登记处的数据。我们纳入了所有将家庭医生、产科医生或助产士列为 MRP 的分娩(=425 056),并根据改良的围产期风险评分系统按妊娠风险状况(低、中或高)对分析进行分层。我们通过计算调整后的绝对和相对风险来估计 MRP 组之间结局的差异。
与选择医生作为 MRP 的客户相比,在各个医疗风险阶层中选择助产士护理的客户的不良新生儿结局的调整后绝对和相对风险均较低。助产士客户的自然阴道分娩、剖宫产术后阴道分娩和母乳喂养起始率更高,剖宫产率和器械分娩率更低,且不良新生儿结局没有增加。我们发现,与产科医生作为 MRP 相比,高危分娩的助产士客户中催产素引产的风险增加。
我们的研究结果表明,与不列颠哥伦比亚省的其他提供者相比,助产士为具有不同医疗风险水平的客户提供安全的初级保健。未来的研究可能会研究不同的实践和薪酬模式如何影响临床结局、客户和提供者的体验以及医疗保健系统的成本。