Department of Surgical Sciences, Section of Vascular Surgery, Uppsala University, Uppsala, Sweden.
Centre for Research and Development, Uppsala University, Region Gävleborg, Gävle, Sweden.
Br J Surg. 2023 Mar 30;110(4):489-497. doi: 10.1093/bjs/znad030.
The aim of this population-based cohort study was to assess the association between aortic morphological baseline factors in 65-year-old men with subaneurysmal aortic diameter (25-29 mm) and risk of later progression to abdominal aortic aneurysm (AAA) generally considered to be at a diameter for repair (at least 55 mm).
Men with a screening-detected subaneurysmal aorta between 2006 and 2015 in mid-Sweden were re-examined using ultrasonography after 5 and 10 years. Cut-off values for baseline subaneurysmal aortic diameter, aortic size index, aortic height index, and relative aortic diameter (with respect to proximal aorta) were analysed using receiver operating characteristic (ROC) curves, and their associations with progression to AAA diameter at least 55 mm evaluated by means of Kaplan-Meier curves and a multivariable Cox proportional hazard analysis adjusted for traditional risk factors.
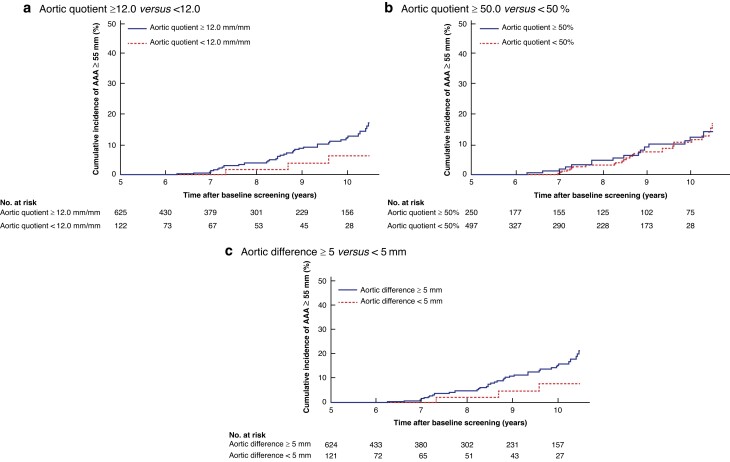
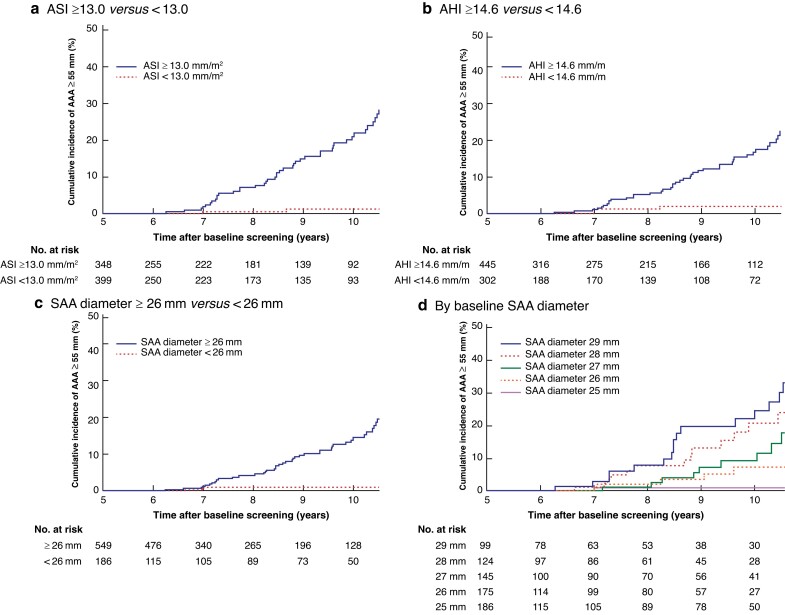
Some 941 men with a subaneurysmal aorta and median follow-up of 6.6 years were identified. The cumulative incidence of AAA diameter at least 55 mm at 10.5 years was 28.5 per cent for an aortic size index of 13.0 mm/m2 or more (representing 45.2 per cent of the population) versus 1.1 per cent for an aortic size index of less than 13.0 mm/m2 (HR 9.1, 95 per cent c.i. 3.62 to 22.85); 25.8 per cent for an aortic height index of at least 14.6 mm/m (58.0 per cent of the population) versus 2.0 per cent for an aortic height index of less than 14.6 mm/m (HR 5.2, 2.23 to 12.12); and 20.7 per cent for subaneurysmal aortic diameter 26 mm or greater (73.6 per cent of the population) versus 1.0 per cent for a diameter of less than 26 mm (HR 5.9, 1.84 to 18.95). Relative aortic diameter quotient (HR 1.2, 0.54 to 2.63) and difference (HR 1.3, 0.57 to 3.12) showed no association with development of AAA of 55 mm or greater.
Baseline subaneurysmal aortic diameter, aortic size index, and aortic height index were all independently associated with progression to AAA at least 55 mm, with aortic size index as the strongest predictor, whereas relative aortic diameter was not. These morphological factors may be considered for stratification of follow-up at initial screening.
本基于人群的队列研究旨在评估 65 岁男性亚AAA 主动脉直径(25-29mm)的主动脉形态基线因素与后期进展为AAA(一般认为直径至少为 55mm 需修复)的风险之间的关联。
2006 年至 2015 年间,在瑞典中部通过筛查发现了亚AAA 主动脉的男性患者,在 5 年和 10 年后使用超声进行复查。使用受试者工作特征(ROC)曲线分析基线亚AAA 主动脉直径、主动脉大小指数、主动脉高度指数和相对主动脉直径(相对于近端主动脉)的截断值,并使用 Kaplan-Meier 曲线和多变量 Cox 比例风险分析评估与至少 55mm 的 AAA 直径进展的关系,该分析调整了传统危险因素。
确定了 941 名患有亚 AAA 主动脉且中位随访时间为 6.6 年的男性患者。10.5 年时,主动脉大小指数≥13.0mm/m2(代表人群的 45.2%)的患者中 AAA 直径至少为 55mm 的累积发生率为 28.5%,而主动脉大小指数<13.0mm/m2 的患者中 AAA 直径至少为 55mm 的累积发生率为 1.1%(HR 9.1,95%CI 3.62 至 22.85);主动脉高度指数≥14.6mm/m 的患者中 AAA 直径至少为 55mm 的累积发生率为 25.8%(代表人群的 58.0%),而主动脉高度指数<14.6mm/m 的患者中 AAA 直径至少为 55mm 的累积发生率为 2.0%(HR 5.2,2.23 至 12.12);亚 AAA 主动脉直径≥26mm 的患者中 AAA 直径至少为 55mm 的累积发生率为 20.7%(代表人群的 73.6%),而亚 AAA 主动脉直径<26mm 的患者中 AAA 直径至少为 55mm 的累积发生率为 1.0%(HR 5.9,1.84 至 18.95)。相对主动脉直径商(HR 1.2,0.54 至 2.63)和差值(HR 1.3,0.57 至 3.12)与 55mm 或更大的 AAA 的发展均无关联。
基线亚 AAA 主动脉直径、主动脉大小指数和主动脉高度指数均与至少 55mm 的 AAA 进展独立相关,其中主动脉大小指数是最强的预测因素,而相对主动脉直径则不然。这些形态学因素可在初始筛查时考虑用于分层随访。